METHODS AND DEVICES FOR VEIN HARVESTING
The present application claims the benefit of and priority to U.S. Provisional Application Ser. No. 62/063,492, filed on Oct. 14, 2014, the entire contents of which are incorporated herein by reference. The present disclosure relates to methods and devices for endoscopic surgery, in particular to methods and devices for dissecting tissue to create a working space for endoscopic instruments. Numerous surgical procedures have been developed to replace veins and arteries that have become blocked by disease. As a result of aging and/or disease, veins and arteries may become blocked by plaque deposits, stenosis, or cholesterol. In some instances, these blockages can be treated with artherectomy, angioplasty or stent placement, and coronary bypass surgery is not required. Coronary bypass surgery is required when these other methods of treatment cannot be used or have failed to clear the blocked vein or artery. In the coronary bypass surgery, a vein is harvested from elsewhere in the body and grafted into place (e.g., between the aorta and the coronary artery) beyond the point of blockage. The coronary bypass surgery requires a length of vein or artery for the graft. It is preferred to use a vein taken from the patient undergoing the bypass surgery. The patient is a ready source of suitable veins that will not likely be rejected by the body after transplantation and grafting onto the aorta and coronary artery. The saphenous vein in the leg is often the best substitute for small veins or arteries such as the coronary arteries, and it is often the preferred vein for use in coronary bypass surgery. This is because the saphenous vein is typically 3 to 5 mm in diameter, about the same size as the coronary arteries. Also, the venous system of the legs is sufficiently redundant so that after removal of the saphenous vein, other veins that remain in the leg are adequate to provide adequate blood flow. The cephalic vein in the arm is an alternative that is sometimes used. In a typical operation previously required to harvest the saphenous vein, the surgeon cut into the leg to allow access to the saphenous vein and cut the vein from the leg. To expose the vein, the surgeon makes a series of incisions from the groin to the knee or the ankle leaving one or more skin bridges along the line of the incisions. (Some surgeons make one continuous incision from the groin to the knee or ankle). Handling of the vein must be kept to a minimum, but the vein must be removed from connective tissue, which requires some force. After exposing the vein, the surgeon grasps it with his fingers while stripping off the surrounding tissues with dissecting scissors or other scraping instruments. The surgeon uses his fingers and blunt dissection tools to pull and lift (or mobilize) the vein from the surrounding tissue. The vein is mobilized or pulled as far as possible through each incision. To reach under the skin bridges, the surgeon lifts the skin with retractors and digs the vein free. While stripping the vein, the surgeon will encounter the various tributary veins that feed into the saphenous vein. These tributaries must be ligated and divided. To divide and ligate tributaries that lie under the skin bridges, the surgeon may need to cut one end of the saphenous vein and pull it under the skin bridge to gently pull the vein out from under the skin bridge until the tributary is sufficiently exposed so that it may be ligated and divided. When the vein has been completely mobilized, the surgeon cuts the proximal and distal ends of the vein and removes the vein from the leg. After removal, the vein is prepared for implantation into the graft site, and the long incisions made in the leg are stitched closed. The procedure described above can also be used to harvest veins for a femoral popliteal bypass, in which an occluded femoral artery is bypassed from above the occlusion to the popliteal artery above or below the knee. The procedure can also be used to harvest veins for the revascularization of the superior mesenteric artery which supplies blood to the abdominal cavity and intestines. In this case, the harvested vein is inserted between the aorta to the distal and patent (unblocked) section of the mesenteric artery. For bypass grafts of the lower popliteal branches in the calf, the procedure can be used to harvest the umbilical vein. The harvested vein can also be used for a vein loop in the arm (for dialysis) between the cephalic vein and brachial artery. The procedures may be used also to harvest veins for femoral-tibial, femora-peroneal, aorto-femoral, and iliac-femoral bypass operations and any other bypass operation. As can be seen from the description of the harvesting operation, the harvesting operation is very traumatic in its own right. In the case of coronary artery bypass, this operation is carried out immediately before the open chest operation required to graft the harvested vein onto the coronary arteries. The vein harvesting operation is often the most troublesome part of the operation. The long incisions created in the leg can be slow to heal and very painful. Complications resulting from the vein harvesting operation can also hinder the patient's recovery from the entire operation. Additionally, during the harvesting of the saphenous vein, it is often desirable to leave as much of the pedicle (i.e., between about 4 mm and about 5 mm of perivascular fat surrounding the vein) preserved as possible. The preservation of the pedicle helps the saphenous vein remain uninjured during surgery, and also helps the long-term patency and viability of the saphenous vein. For instance, following the surgery, the pedicle acts as a natural sheath to help prevent the saphenous vein from getting unnaturally distended due to higher arterial pressures. The method of vein harvesting presented herein is accomplished with endoscopic procedures while preserving much of the pedicle. This allows the vein to be harvested in an operation that requires only a few small incisions, and increases the patency of the vein. Endoscopic surgical techniques for operations such as gall bladder removal and hernia repair are now common. The surgeon performing the operation makes a few small incisions and inserts long tools, including forceps, scissors, and staplers into the incision and deep into the body. Viewing the tools through an endoscope, or a video display from an endoscope, the surgeon can perform all the cutting and suturing operations necessary for a wide variety of operations. The procedures are also referred to as endoscopic surgery, laparoscopic surgery, minimally invasive surgery, or video-assisted surgery. References to endoscopic surgery and endoscopes below is intended to encompass all of these fields, and all operations described below with reference to endoscopes can also be accomplished with laparoscopes, gastroscopes, and any other imaging devices which may be conveniently used. Minimally invasive procedures for vein removal have been proposed. Knighton, Endoscope and Method for Vein Removal, U.S. Pat. No. 5,373,840 shows a method of cutting the saphenous vein at one end, and grasping the vein with graspers or forceps, then sliding a ring over the vein while securing the vein at the same time. Knighton uses a dissecting tool with an annular cutting ring, and requires that the saphenous vein be overrun or progressively surrounded with the dissecting tool and the endoscope, so that after the endoscope has been inserted as far as it will go, the entire dissected portion of the vein has been pulled in the lumen of the endoscope. As shown in FIGS. 1 and 10 of Knighton, the method requires deployment of the forceps inside the annular dissection loop, and it requires deployment of the loop and graspers inside the endoscope lumen. The blood vessel must be cut and grasped by the forceps before it can be dissected by the dissecting ring. The present disclosure relates to a vein harvesting device, comprising a handle assembly, an elongated portion extending distally from the handle assembly and defining a longitudinal axis, an end effector, and a retractor. The end effector is disposed adjacent a distal portion of the elongated portion, and includes a first jaw member and a second jaw member. At least one jaw member is movable toward the other jaw member. The retractor is disposed in mechanical cooperation with the elongated portion, and includes a shaft and a pair of legs. The retractor is movable from a non-deployed position where the shaft is aligned with the longitudinal axis, to a deployed position where the shaft is disposed at an angle with respect to the longitudinal axis. In disclosed aspects, the legs of the retractor are made from a shape memory material. Here, it is disclosed that a distance between the legs of the retractor in the non-deployed position is smaller than the distance between the legs of the retractor in the deployed position. In disclosed aspects, the legs include an inner surface configured for contacting tissue, and wherein the inner surface of the legs includes a non-traumatic material disposed thereon. In disclosed aspects, the retractor is rotatable about the longitudinal axis. In disclosed aspects, the retractor is rotatable about the longitudinal axis independently of the end effector. In disclosed aspects, the end effector is configured to seal tissue. The present disclosure also relates to a method of endoscopically harvesting the saphenous vein and surrounding pedicle. The method comprises using a vein harvesting device including a handle assembly, an elongated portion extending distally from the handle assembly and defining a longitudinal axis, an end effector, and a retractor. The end effector is disposed adjacent a distal portion of the at least one elongated portion, and includes a first jaw member and a second jaw member. At least one jaw member is movable toward the other jaw member. The retractor is disposed in mechanical cooperation with the elongated portion, and includes a shaft and a pair of legs. The method also includes endoscopically inserting at least a portion of the vein harvesting device adjacent the saphenous vein of a patient, sealing and/or cutting tissue with the end effector of the vein harvesting device, deploying the retractor of the vein harvesting device from a non-deployed position where the shaft is aligned with the longitudinal axis, to a deployed position where the shaft is disposed at an angle with respect to the longitudinal axis, positioning the legs of the retractor into contact with at least one the saphenous vein and pedicle to be removed, and removing at least a portion of the saphenous vein and pedicle from the patient. In disclosed aspects of the method, sealing and/or cutting tissue with the end effector of the vein harvesting device includes sealing and/or cutting tissue surrounding the pedicle. In disclosed aspects of the method, the method also includes rotating the retractor about the longitudinal axis. In disclosed aspects of the method, the method also includes rotating the retractor about the longitudinal axis independently of the end effector. Various embodiments of the surgical devices are described herein with reference to the drawings wherein: Embodiments of the presently disclosed vein harvesting device are described in detail with reference to the drawings, in which like reference numerals designate identical or corresponding elements in each of the several views. As used herein the term “distal” refers to that portion of the vein harvesting device that is farther from the user, while the term “proximal” refers to that portion of the vein harvesting device that is closer to the user. The saphenous vein has a number of tributary veins that carry venous blood into the vein. These tributaries are typically tied off and/or cut off of the saphenous vein before the saphenous vein can be removed. In medical terms, these tributaries must be ligated and divided. When a tributary or side branch is encountered, the surgeon can use endoscopic and laparoscopic tools, for example, to close the tributaries and cut them from the saphenous vein. The tributaries can be separated from the vein after the entire vein is stripped, or the surgeon may choose to separate them as they are encountered. Referring initially to Tip or blunt dissection tip 400 extends distally of end effectors 300 Handle assembly 100 is configured to control actuation of end effectors 300 It is further disclosed that first jaw members 310 Additionally, and as shown in the embodiment illustrated in End effectors 300 It is further disclosed that the distance “D” between end effectors 300 Embodiments of vein harvesting device 10 of the present disclosure also include an endoscope disposed between elongated portions 200 It is further envisioned that vein harvesting device 10 includes a hollow cavity between elongated portions 200 Referring now to It is further envisioned that band 500 can be deployed and/or retracted with the use of a control (e.g., switch) on handle assembly 100. Band 500 may initially lie parallel with either first elongated portion 200 It is also disclosed that band 500 (e.g., disposed in a different suitable location) holds the vein “V” either between elongated portions 200 During vein harvesting procedures when a surgeon does not have access to the disclosed vein harvesting device 10 or band 500, the surgeon often either uses his or her finger or hand to hold back the vein “V,” or the surgeon uses a separate instrument including a hook, for example. However, during vein harvesting inclusive of pedicle harvesting, as described herein, the size and weight of the vein/pedicle (as compared to a skeletonized vein without pedicle) impede the use of a finger, hand or hook to hold back the vein/pedicle. Accordingly, band 500 of the present disclosure is especially useful during harvesting of the vein and pedicle. With reference to With particular reference to With particular reference to The present disclosure also includes methods of performing vein harvesting operations using vein harvesting device 10 discussed herein, and methods of manufacturing vein harvesting device 10 discussed herein. Methods and devices presented herein take advantage of laparoscopic procedures to lessen the trauma of vein harvesting operations. Instead of making an incision along or over the entire length, or essentially the entire length of the vein “V” to be harvested, the procedure may be conducted with only a few small incisions or a single incision. All that is needed is a working space large enough to allow the surgeon to use vein harvesting device 10 and view the operation through a laparoscope, for example. In disclosed embodiments of the method, the surgeon creates a working space under the skin and over the saphenous vein using laparoscopic techniques. The surgeon makes one or several small incisions to expose the saphenous vein. These incisions are referred to as cut-downs. A distal incision near the knee and/or a proximal incision at the groin are contemplated. If the entire length of the saphenous vein is to be harvested, an additional incision can be made close to the ankle. The saphenous vein can be seen through the cut-downs. The use of three or four incisions used to harvest the entire saphenous vein are merely a matter of convenience, and those particularly skilled in laparoscopic procedures may require fewer incisions, and also more small incisions may be desired. After the incision(s), the surgeon inserts vein harvesting device 10 into one incision and pushes it along the saphenous vein “V” towards the other incision. The tunneling creates a channel running along the saphenous vein “V.” The channel may be expanded by insertion of a balloon (not shown), which can be inflated to expand or propagate the tunnel further along the saphenous vein A balloon (not shown) may packed inside vein harvesting device 10. The balloon is a non-elastomeric balloon or bladder and may be deployed through a balloon trocar extending along at least a portion of the length of vein harvesting device 10. It is disclosed that when used for tunneling along the saphenous vein “V,” the balloon is approximately 60 centimeters long, and the balloon trocar may be between about 10-20 centimeters long. The balloon can be expanded by injecting liquid or gas into the balloon through an inflation port. Sterile saline solution is an example of an inflation medium for medical applications. Alternately, air, CO2, or even foam or other substances may be injected to cause inflation. Further details of the balloon and its use for harvesting veins are disclosed in U.S. patent application Ser. No. 12/550,462, the entire contents of which being incorporated by reference herein. With reference to Vein harvesting device 1000 includes a handle assembly 1100, an elongated portion 1200 extending distally from handle assembly 1100, an end effector 1300 disposed adjacent a distal end of elongated portion 1200, and a deployable retractor 1400 disposed in mechanical cooperation with elongated portion or endoscopic portion 1200. Handle assembly 1100 is configured to control actuation of end effector 1300 (e.g., pivoting at least one jaw member with respect to the other, and cutting and sealing tissue disposed between the jaw members). Details of a surgical instrument including a handle assembly for controlling actuation of an end effector can be found in U.S. patent application Ser. Nos. 10/179,863 and 10/116,944, the entire contents of which have been incorporated by reference herein. Additionally, handle assembly 1100 is configured to control deployment of retractor 1400 between a first, non-deployed position where a shaft 1410 is aligned with a longitudinal axis “A1-A1” defined by elongated portion 1200 ( In use, when retractor 1400 is deployed ( Retractor 1400 includes the shaft 1410 and a pair of legs 1420, which form a U-like shape. Legs 1420 extend from shaft 1410 and are sized to hold portions of the vein “V” and pedicle “P” therebetween. As such, it is envisioned that the distance “DL” between legs 1420 is between about 10 mm and about 15 mm, however the distance “DL” between legs 1420 may be larger or smaller. Additionally, since it is often desirable in endoscopic surgery to have elongated portion 1200 with a diameter of less than 10 mm, legs 1420 of retractor 1400 may be formed from a shape memory material. Here, when retractor 1400 is in its non-deployed position ( Additionally, the retractor 1400 may be at least partially disposed within a recess of elongated portion 1200 when retractor 1400 is in its non-deployed position, such that the profile of elongated portion 1200 is substantially unchanged by the inclusion of retractor 1400. That is, in such embodiments, retractor 1400 would not increase the overall diameter or profile of elongated portion 1200 (e.g., endoscopic portion), and thus would not hinder the endoscopic use of vein harvesting device 1000. It is further disclosed that at least portions of retractor 1400 include a non-traumatic tissue-contacting surface. For example, at least an inner surface 1422 of legs 1420 may include a non-traumatic material disposed thereon to help prevent damage to the vein “V” or pedicle “P.” Additionally, in disclosed embodiments, retractor 1400 is rotatable about longitudinal axis “A-A,” defined by elongated portion. The retractor 1400 may be rotatable about longitudinal axis “A-A” independently of rotation of end effector 1300, which may also be rotatable about longitudinal axis “A-A.” Rotation of retractor 1400 may be accomplished by the rotation of a knob 1430 located in mechanical cooperation with handle assembly 1100. Knob 1430 may be mechanically linked to the portion of shaft 1410 that extends from elongated portion 1200. The various embodiments disclosed herein may also be configured to work with robotic surgical systems and what is commonly referred to as “Telesurgery.” Such systems employ various robotic elements to assist the surgeon in the operating theatre and allow remote operation (or partial remote operation) of surgical instrumentation. Various robotic arms, gears, cams, pulleys, electric and mechanical motors, etc. may be employed for this purpose and may be designed with a robotic surgical system to assist the surgeon during the course of an operation or treatment. Such robotic systems may include remotely steerable systems, automatically flexible surgical systems, remotely flexible surgical systems, remotely articulating surgical systems, wireless surgical systems, modular or selectively configurable remotely operated surgical systems, etc. The robotic surgical systems may be employed with one or more consoles that are next to the operating theater or located in a remote location. In this instance, one team of surgeons or nurses may prepare the patient for surgery and configure the robotic surgical system with one or more of the instruments disclosed herein, while another surgeon (or group of surgeons) remotely control the instruments via the robotic surgical system. As can be appreciated, a highly skilled surgeon may perform multiple operations in multiple locations without leaving his/her remote console which can be both economically advantageous and a benefit to the patient or a series of patients. The robotic arms of the surgical system are typically coupled to a pair of master handles by a controller. The handles can be moved by the surgeon to produce a corresponding movement of the working ends of any type of surgical instrument (e.g., end effectors, graspers, knifes, scissors, etc.) which may complement the use of one or more of the embodiments described herein. The movement of the master handles may be scaled so that the working ends have a corresponding movement that is different (smaller or larger) than the movement performed by the operating hands of the surgeon. The scale factor or gearing ratio may be adjustable so that the operator can control the resolution of the working ends of the surgical instrument(s). The master handles may include various sensors to provide feedback to the surgeon relating to various tissue parameters or conditions, e.g., tissue resistance due to manipulation, cutting or otherwise treating, pressure by the instrument onto the tissue, tissue temperature, tissue impedance, etc. As can be appreciated, such sensors provide the surgeon with enhanced tactile feedback simulating actual operating conditions. The master handles may also include a variety of different actuators for delicate tissue manipulation or treatment further enhancing the surgeon's ability to mimic actual operating conditions. While several embodiments of the disclosure have been shown in the drawings, it is not intended that the disclosure be limited thereto, as it is intended that the disclosure be as broad in scope as the art will allow and that the specification be read likewise. Therefore, the above description should not be construed as limiting, but merely as exemplifications of various embodiments. Those skilled in the art will envision other modifications within the scope and spirit of the claims appended hereto. A vein harvesting device is disclosed. The vein harvesting device includes a handle assembly, an elongated portion extending distally from the handle assembly and defining a longitudinal axis, an end effector, and a retractor. The end effector is disposed adjacent a distal portion of the elongated portion, and includes a first jaw member and a second jaw member. At least one jaw member is movable toward the other jaw member. The retractor is disposed in mechanical cooperation with the elongated portion, and includes a shaft and a pair of legs. The retractor is movable from a non-deployed position where the shaft is aligned with the longitudinal axis, to a deployed position where the shaft is disposed at an angle with respect to the longitudinal axis. 1. A vein harvesting device, comprising:
a handle assembly; an elongated portion extending distally from the handle assembly and defining a longitudinal axis; an end effector disposed adjacent a distal portion of the elongated portion, the end effector including a first jaw member and a second jaw member, at least one jaw member movable toward the other jaw member; and a retractor disposed in mechanical cooperation with the elongated portion, the retractor including a shaft and a pair of legs, the retractor movable from a non-deployed position where the shaft is aligned with the longitudinal axis, to a deployed position where the shaft is disposed at an angle with respect to the longitudinal axis. 2. The vein harvesting device of 3. The vein harvesting device of 4. The vein harvesting device of 5. The vein harvesting device of 6. The vein harvesting device of 7. The vein harvesting device of 8. A method of endoscopically harvesting the saphenous vein and surrounding pedicle, the method comprising:
using a vein harvesting device including:
a handle assembly; an elongated portion extending distally from the handle assembly and defining a longitudinal axis; an end effector disposed adjacent a distal portion of the elongated portion, the end effector including a first jaw member and a second jaw member, at least one jaw member movable toward the other jaw member; and a retractor disposed in mechanical cooperation with the elongated portion, the retractor including a shaft and a pair of legs; endoscopically inserting at least a portion of the vein harvesting device adjacent the saphenous vein of a patient; at least one of sealing and cutting tissue with the end effector of the vein harvesting device; deploying the retractor of the vein harvesting device from a non-deployed position where the shaft is aligned with the longitudinal axis, to a deployed position where the shaft is disposed at an angle with respect to the longitudinal axis; positioning the legs of the retractor into contact with at least one the saphenous vein and pedicle to be removed; and removing at least a portion of the saphenous vein and pedicle from the patient. 9. The method of 10. The method of 11. The method of 12. The method of CROSS REFERENCE TO RELATED APPLICATION
BACKGROUND
TECHNICAL FIELD
SUMMARY
BRIEF DESCRIPTION OF THE DRAWINGS
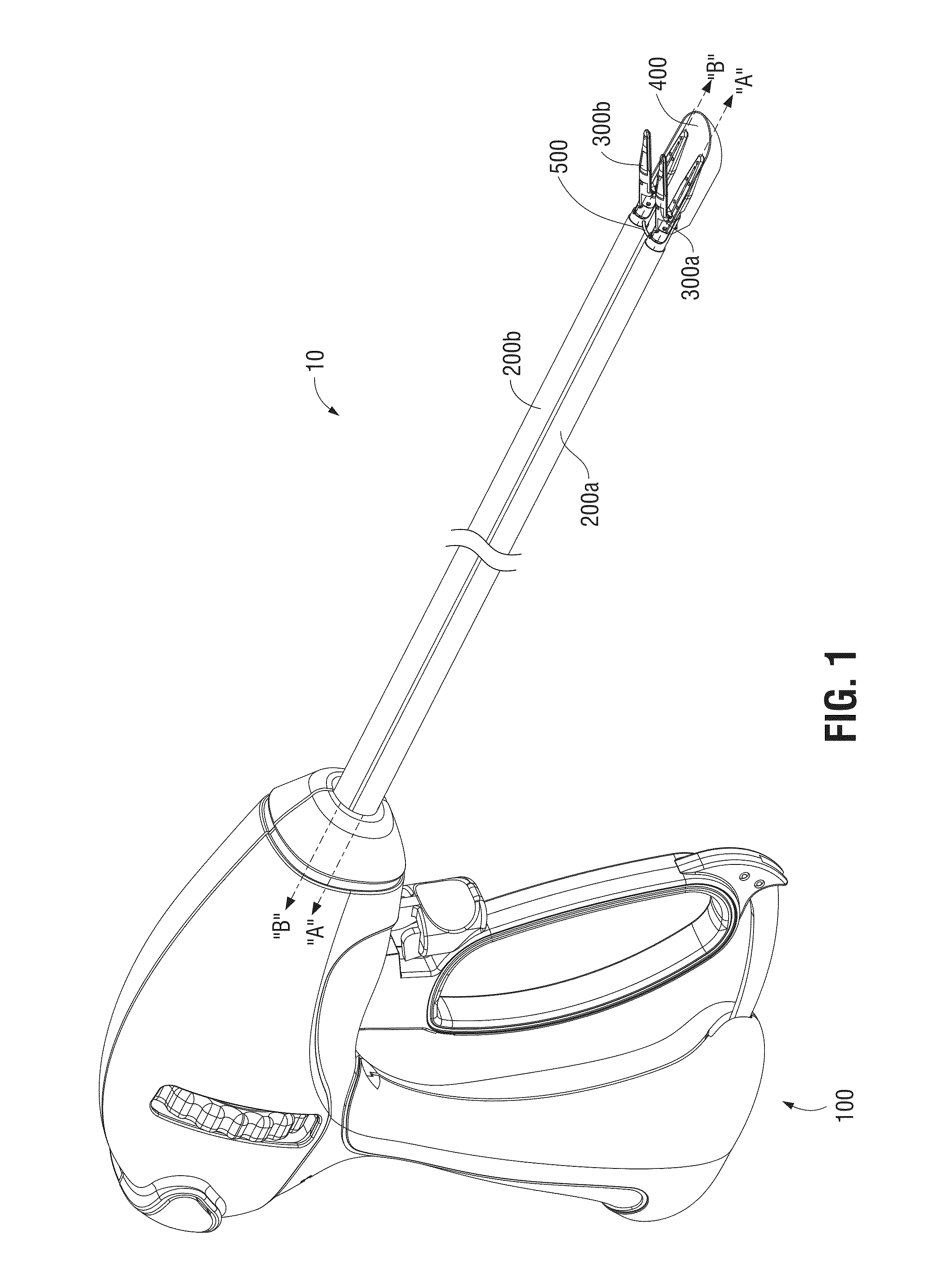
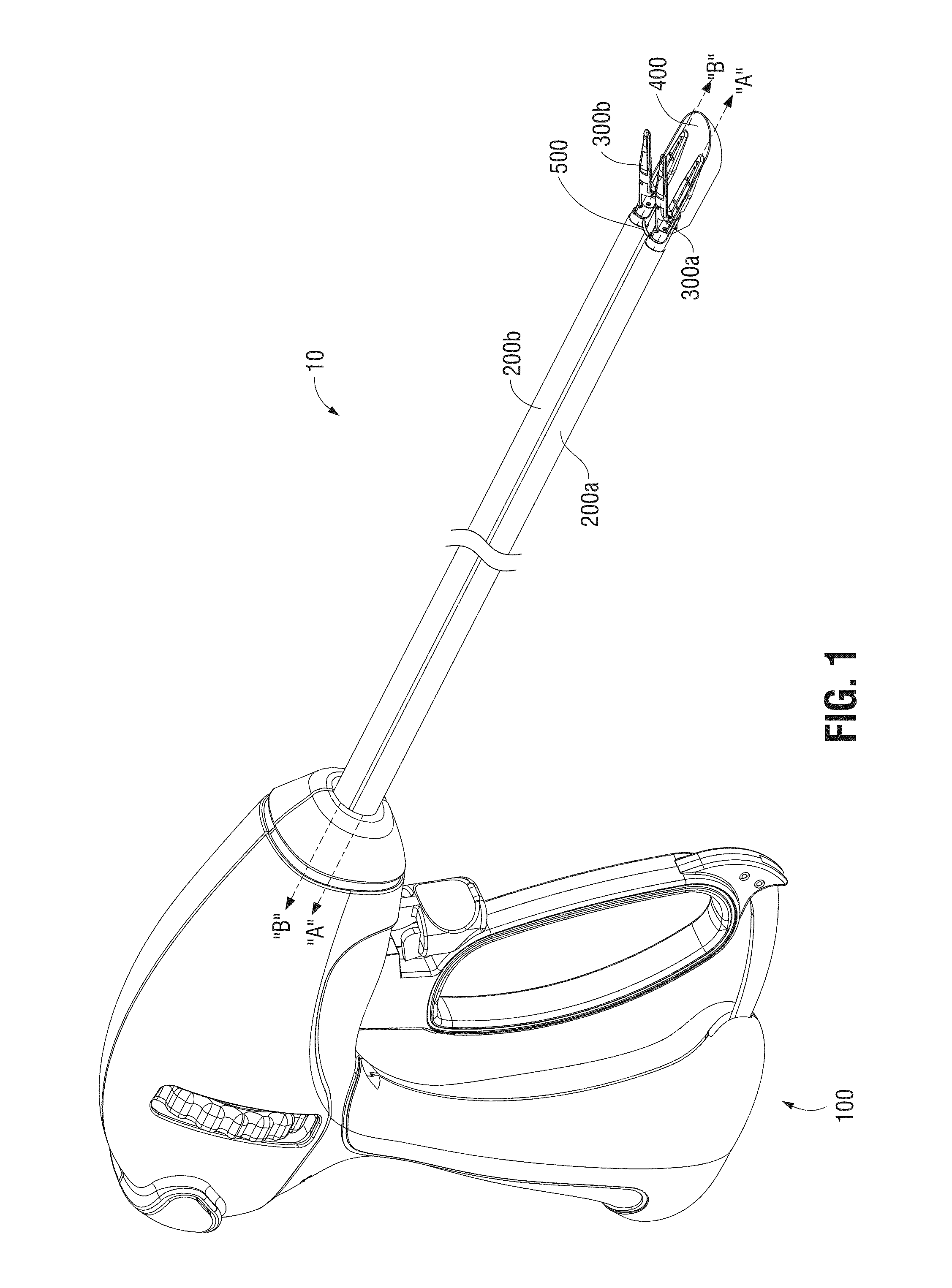
DETAILED DESCRIPTION