DEVICES AND METHODS FOR DELIVERING AN ENDOCARDIAL DEVICE
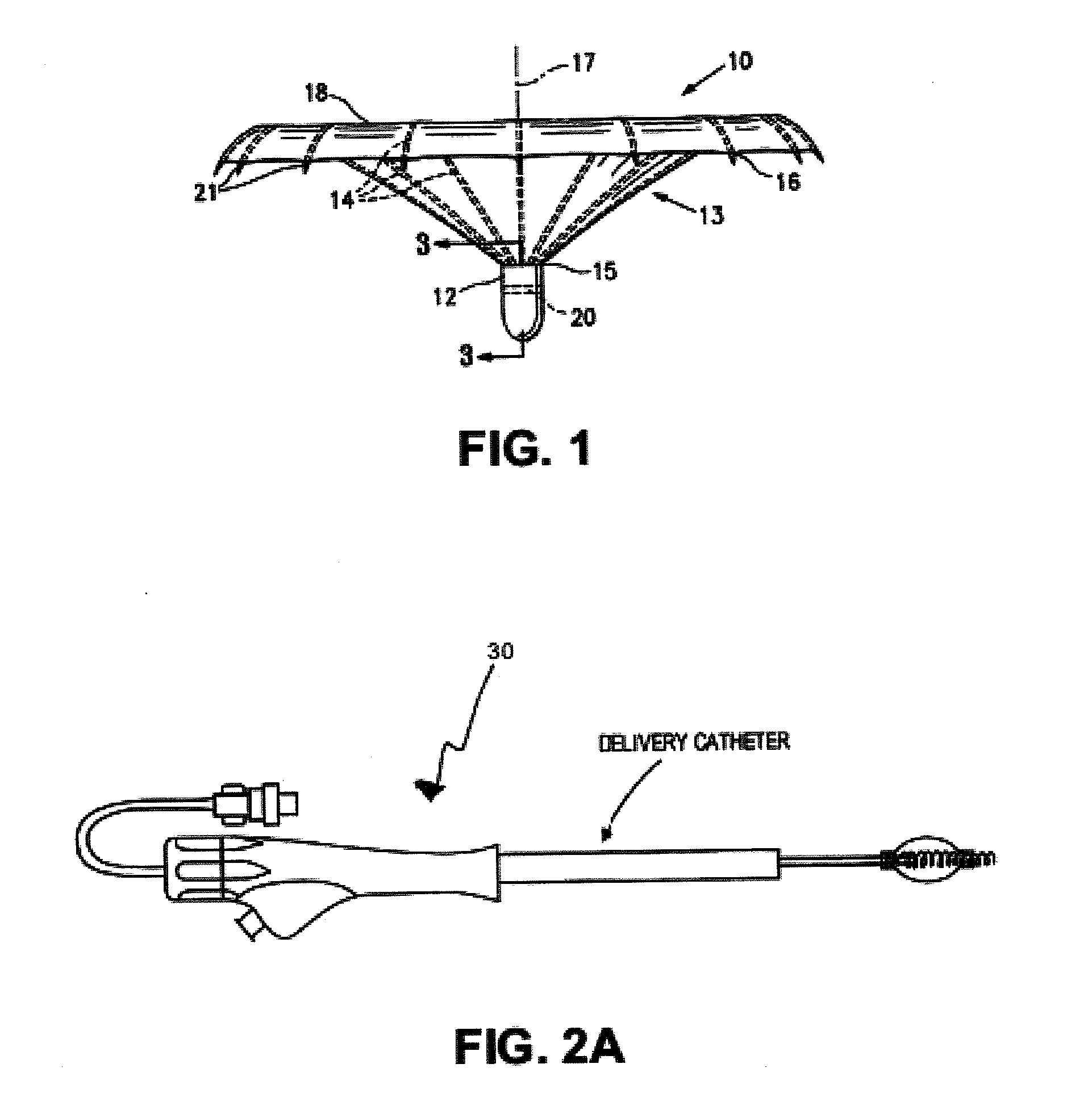
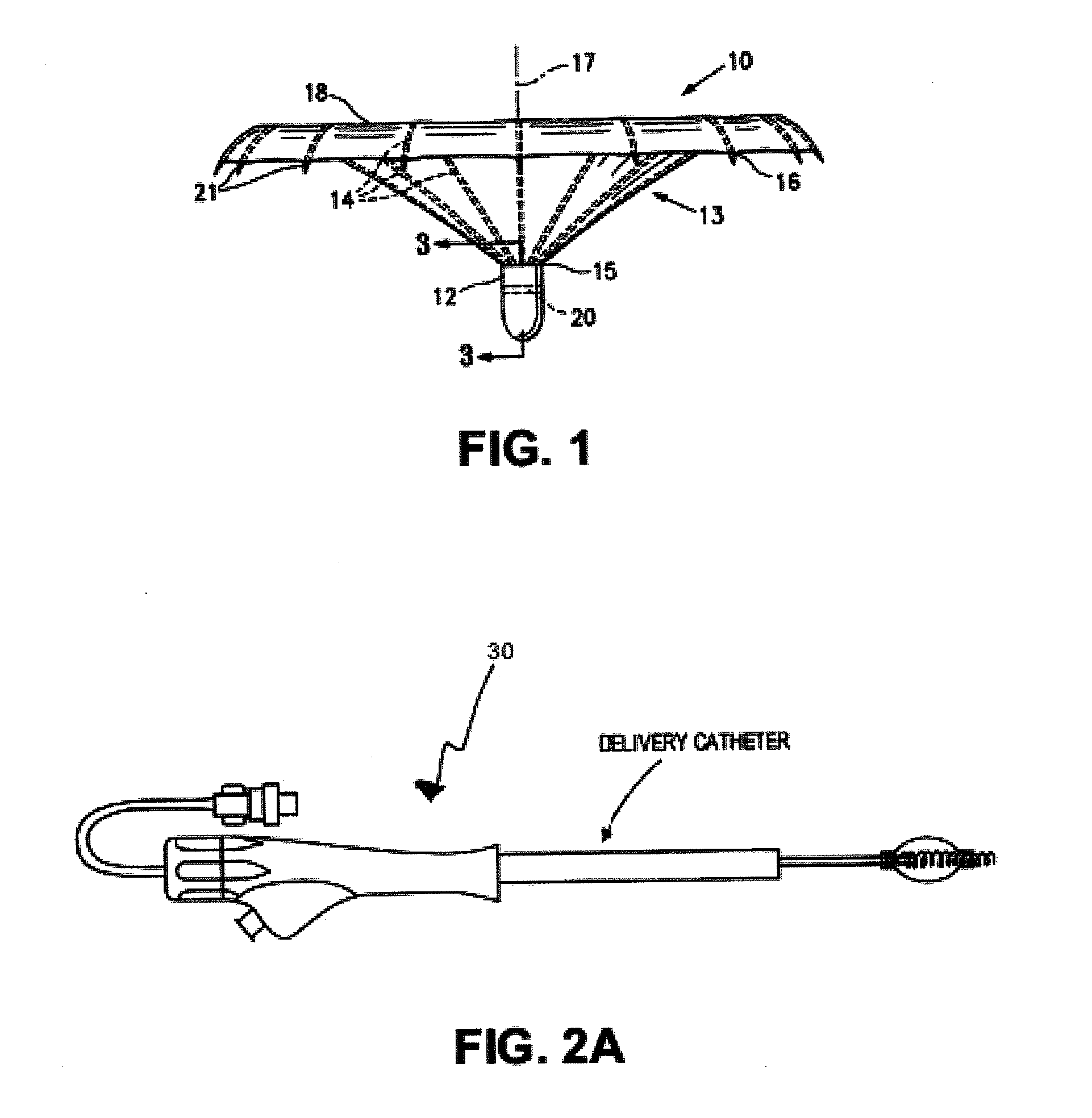
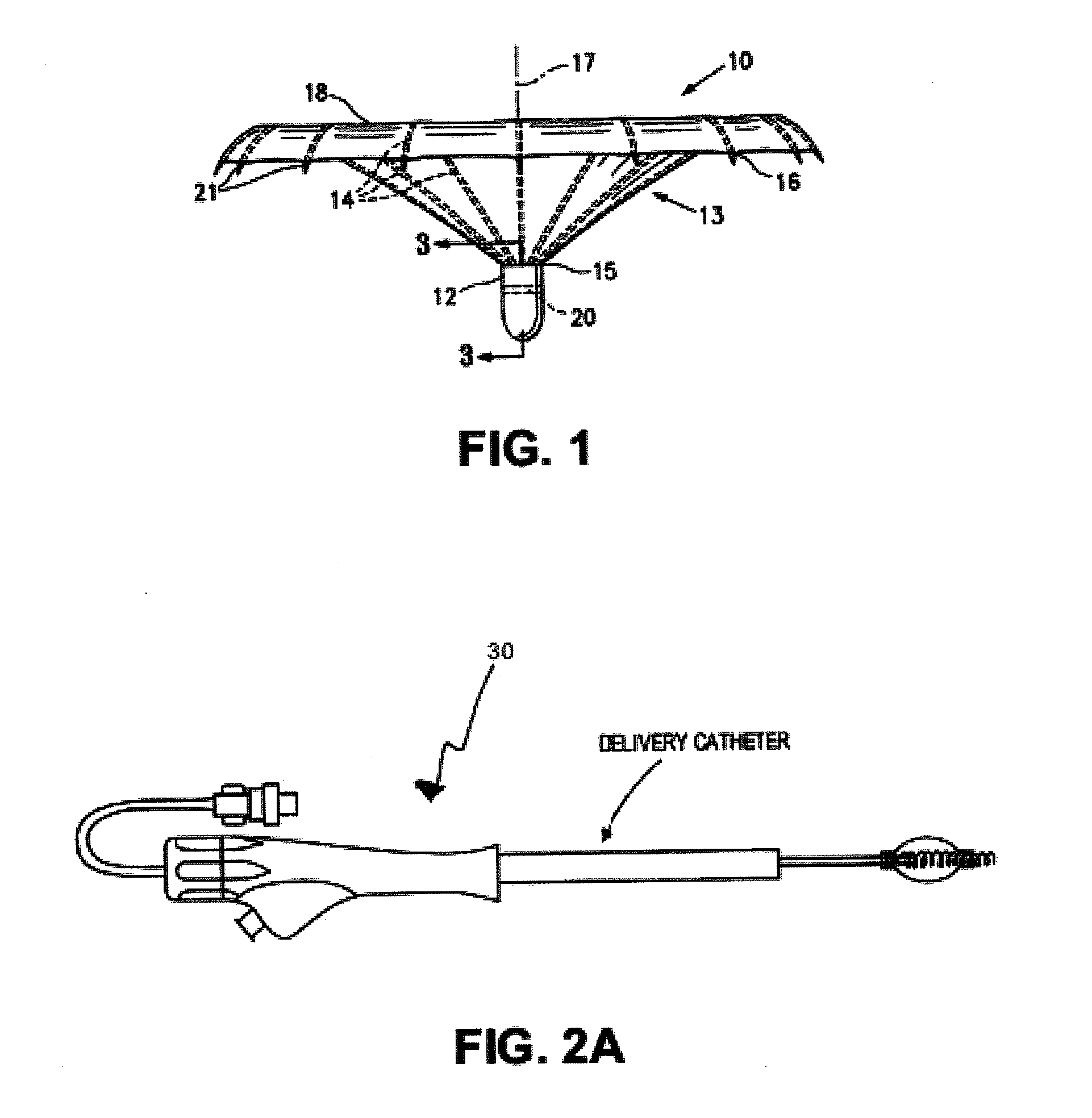
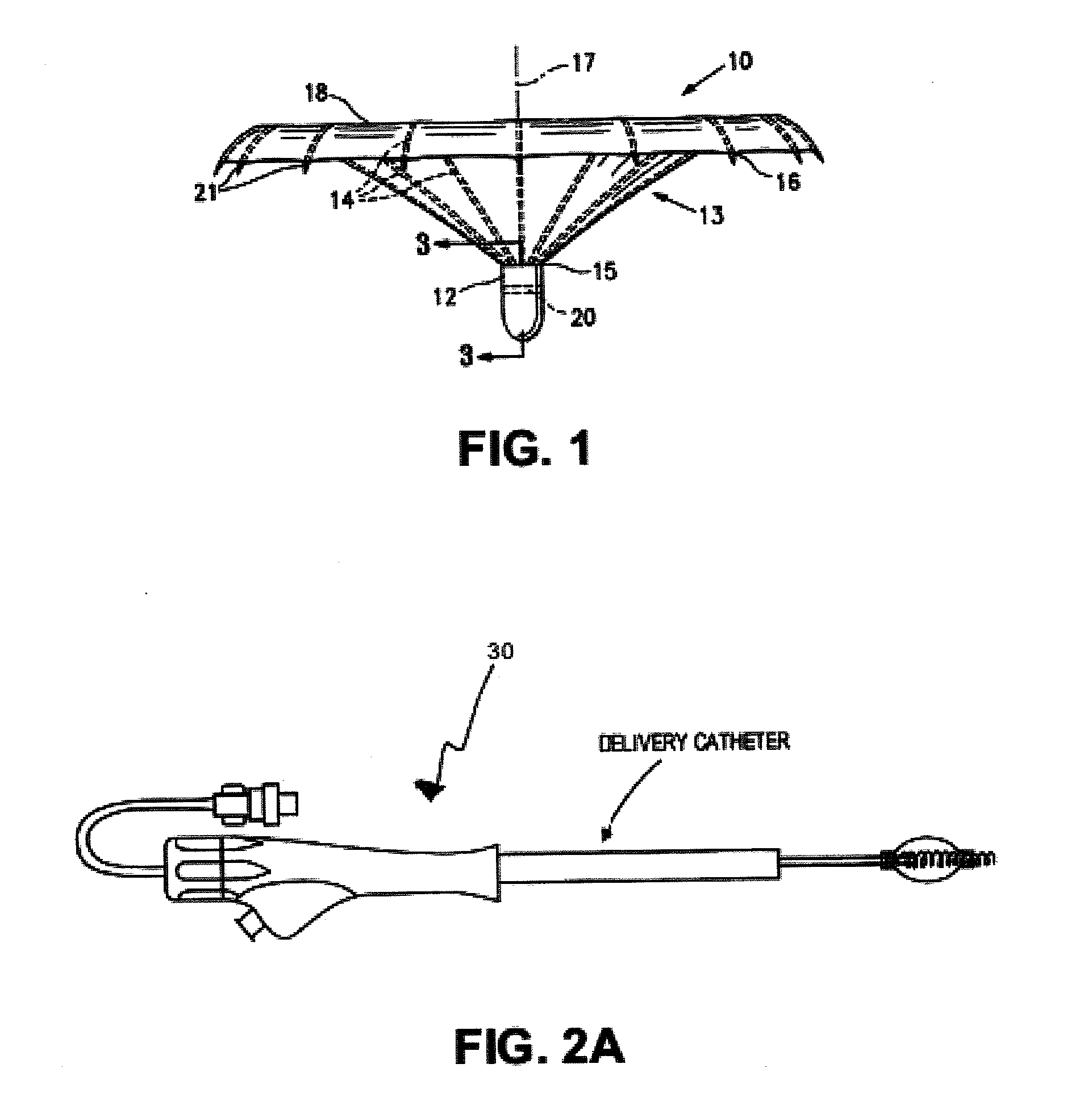
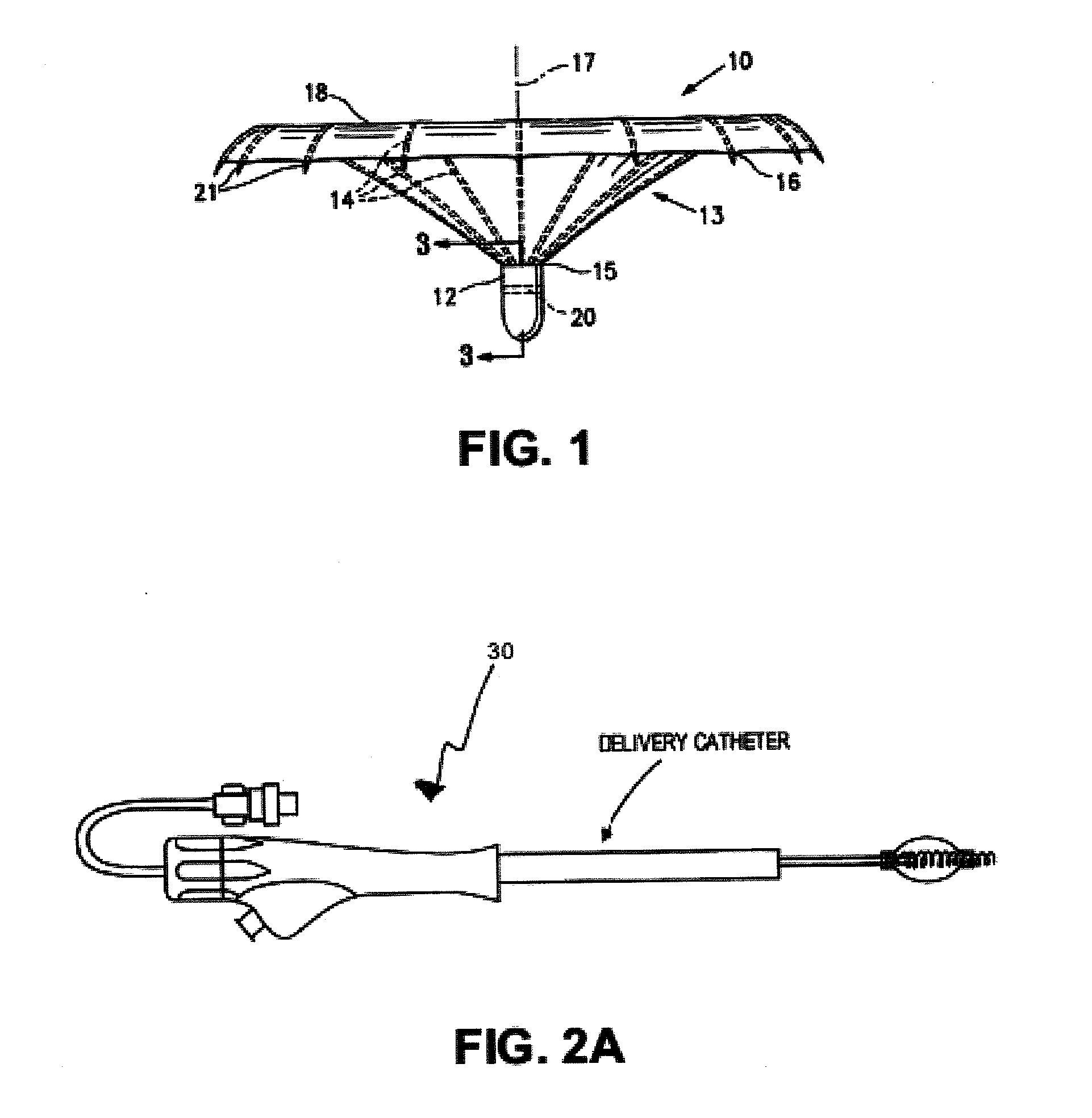
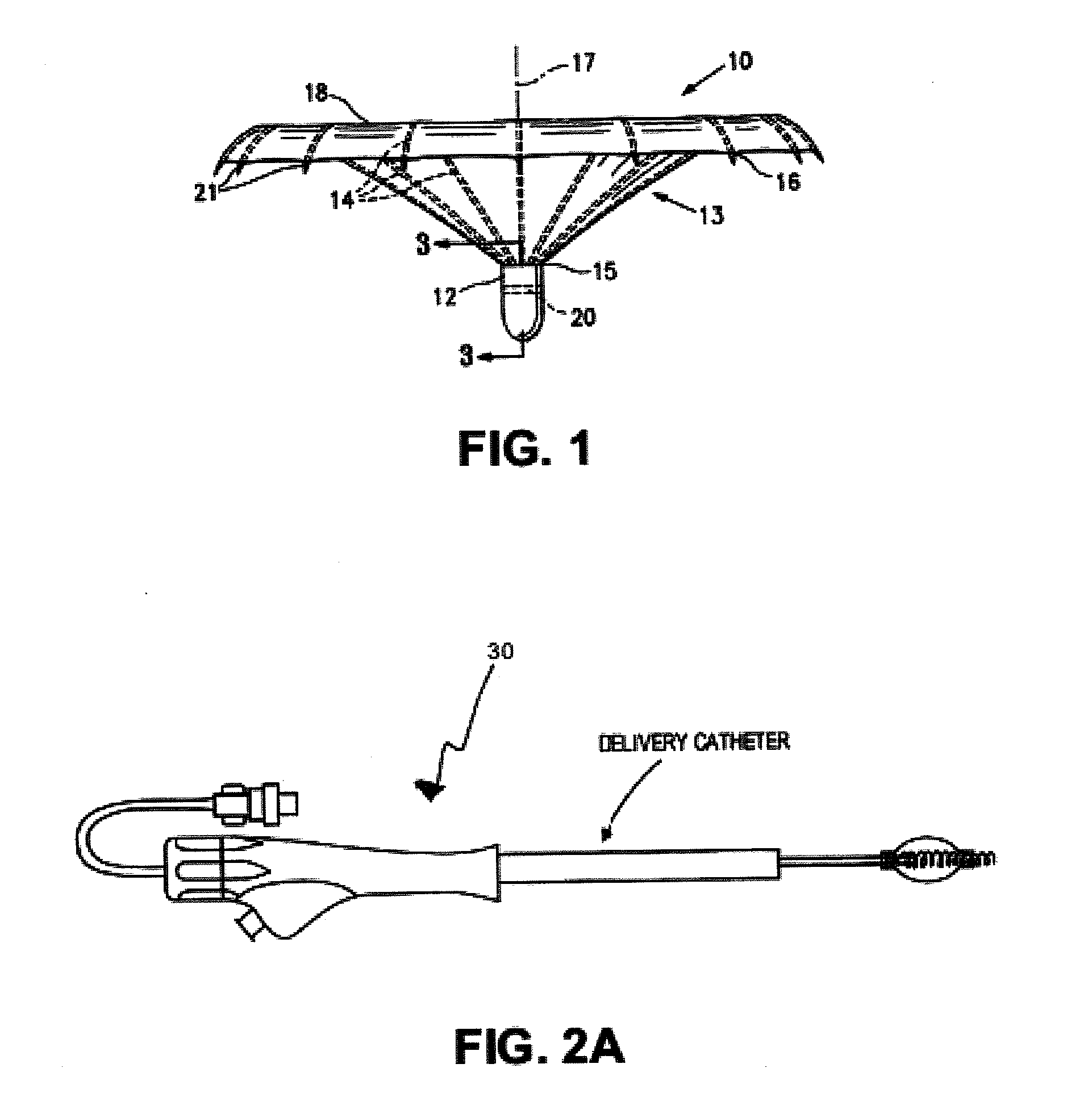
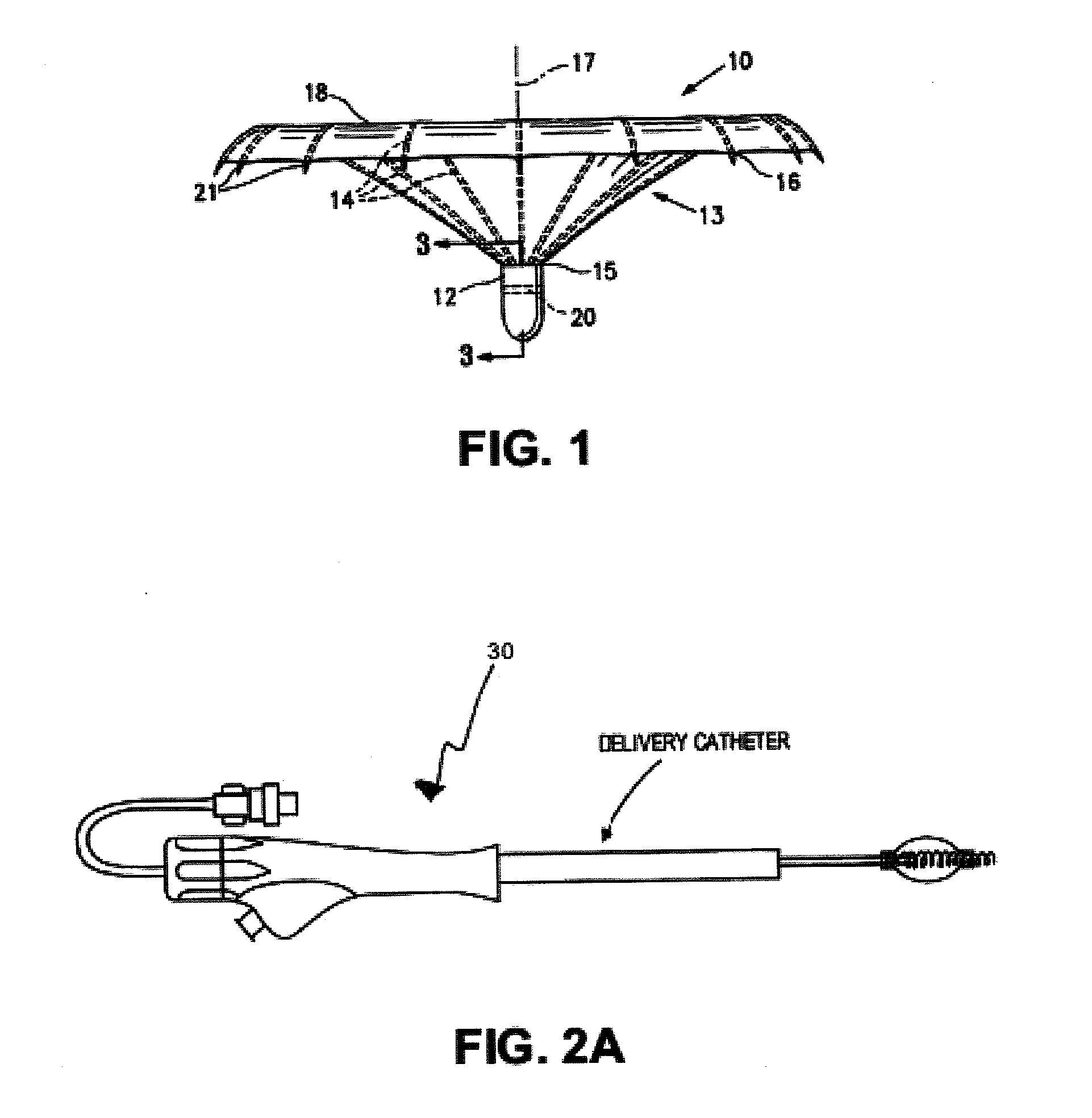
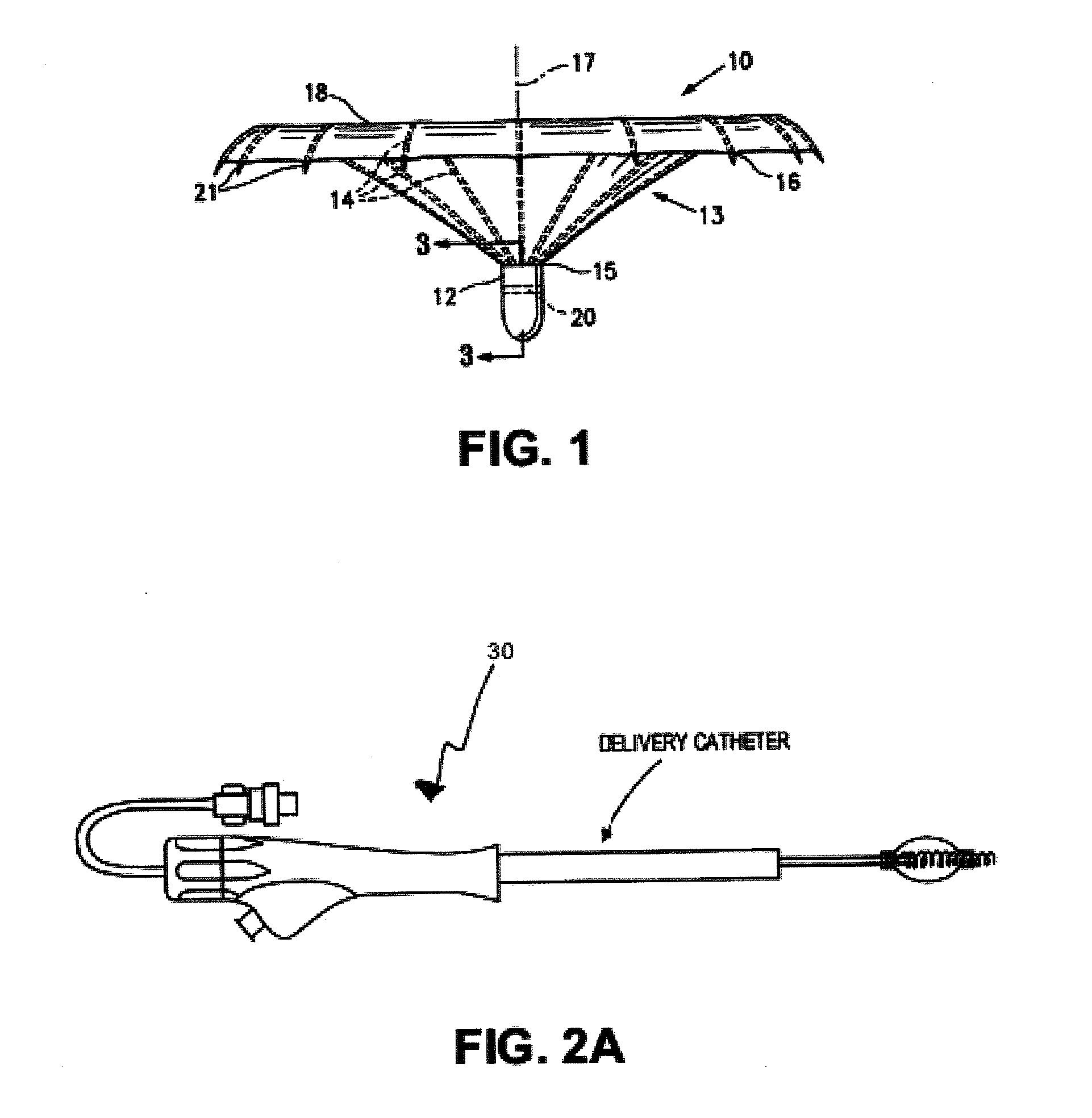
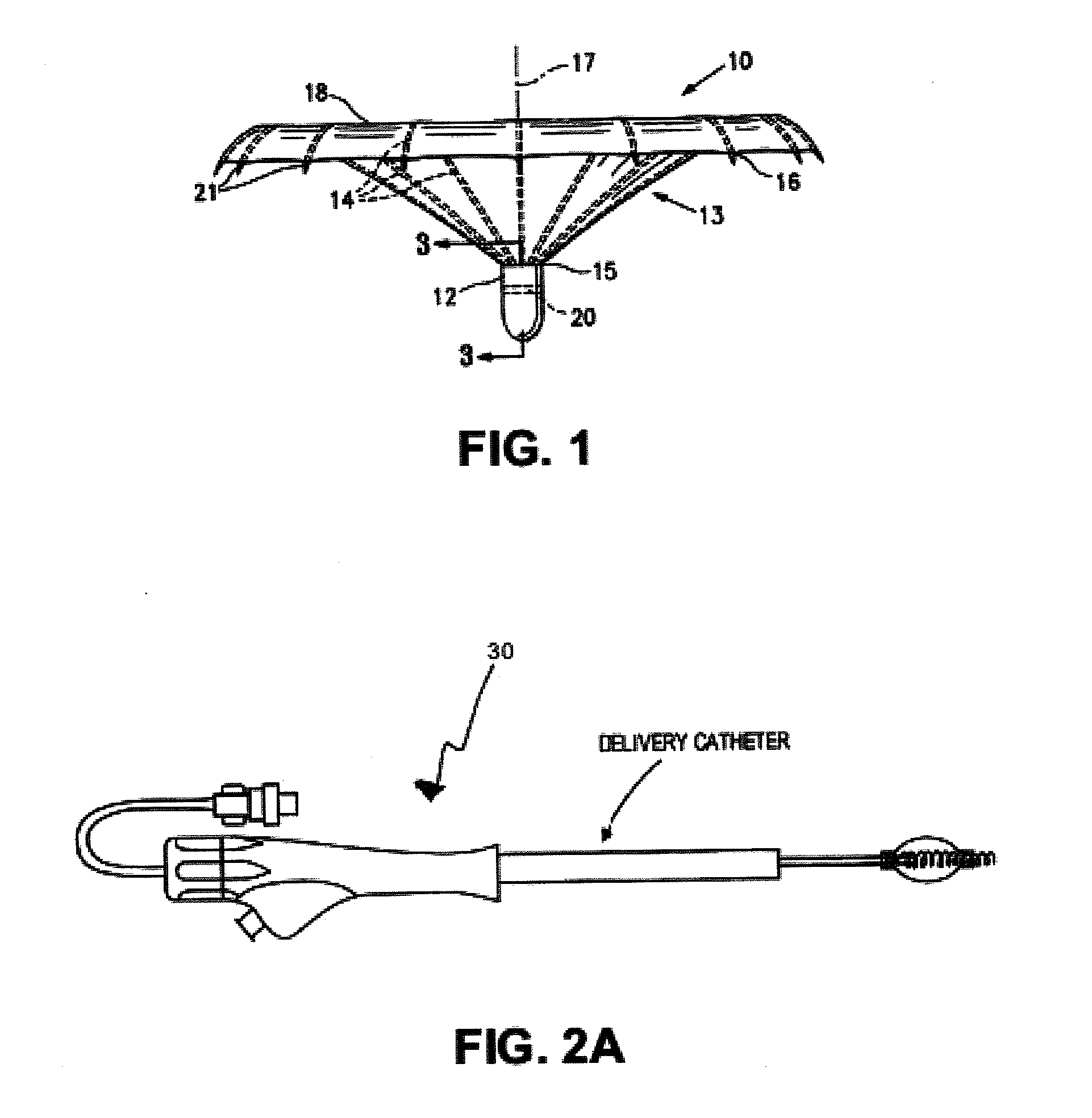
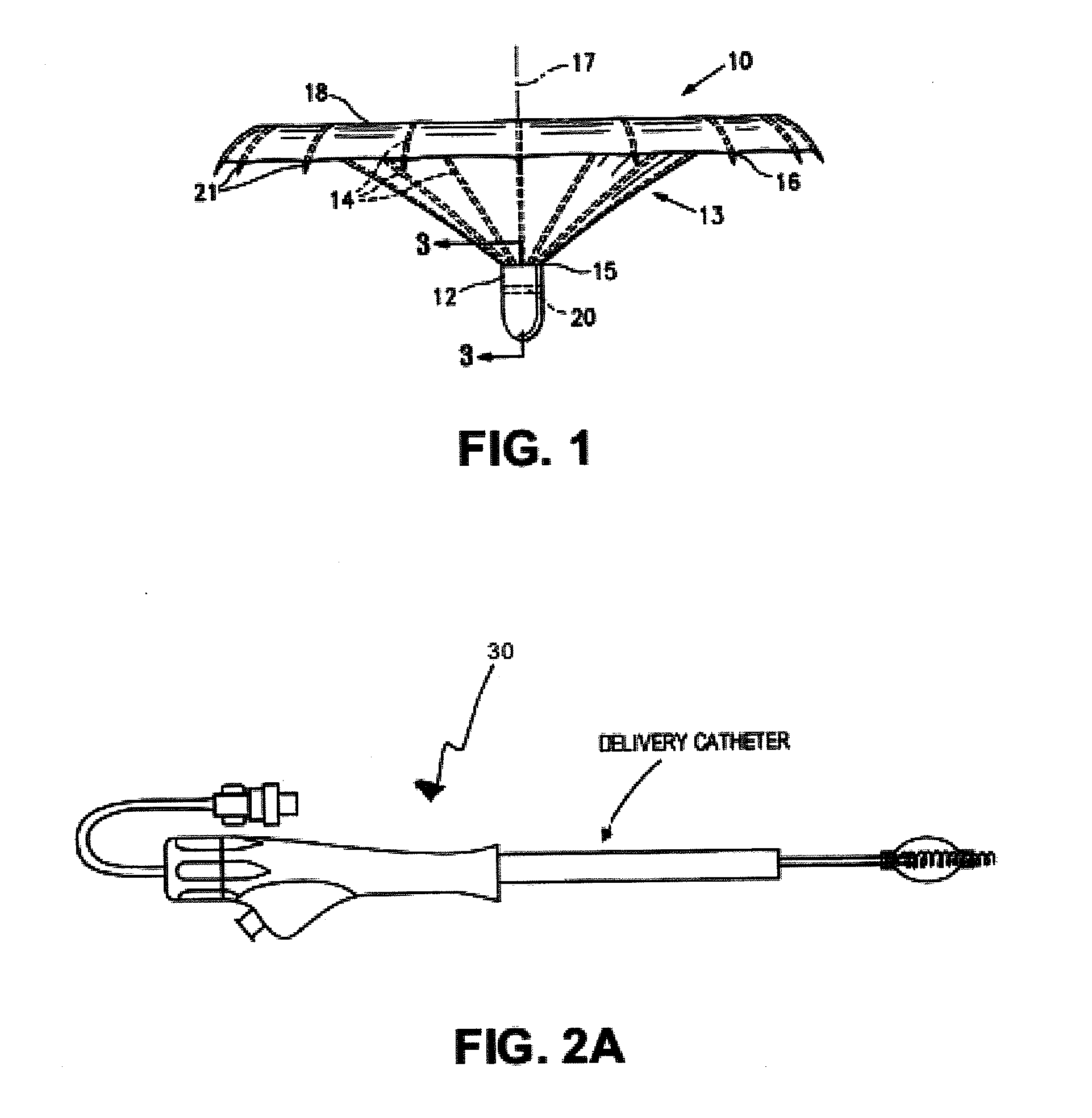
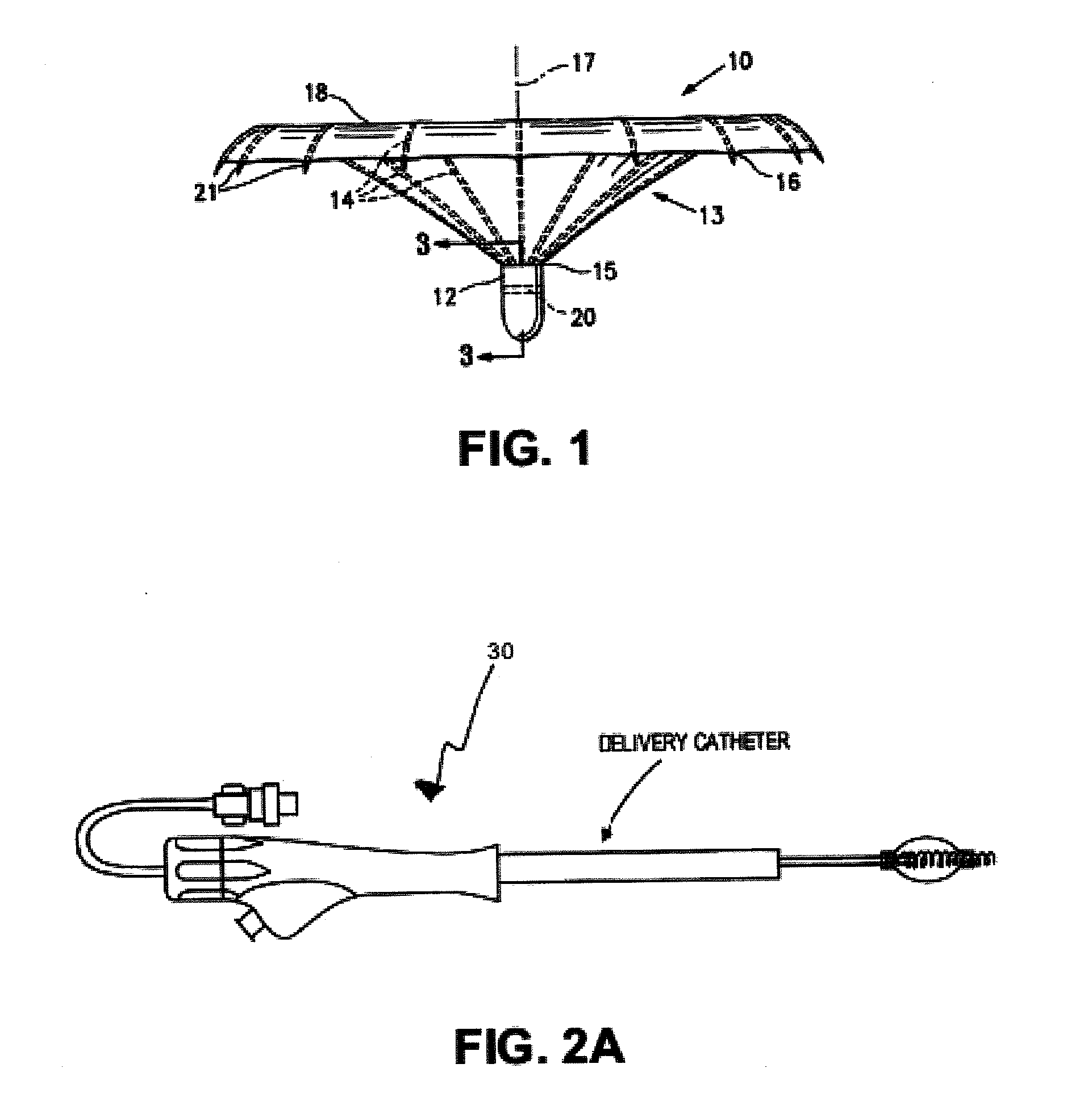
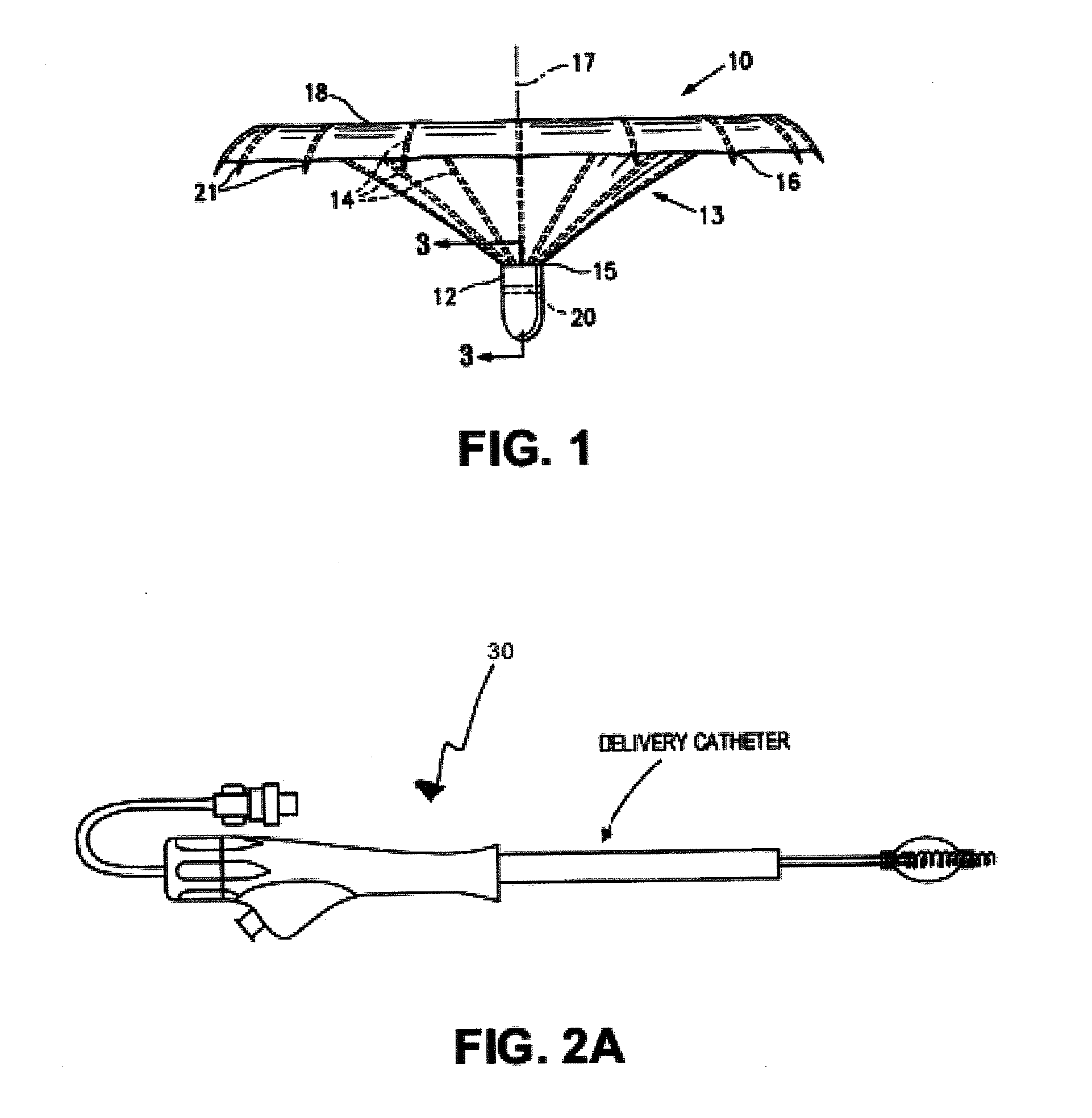
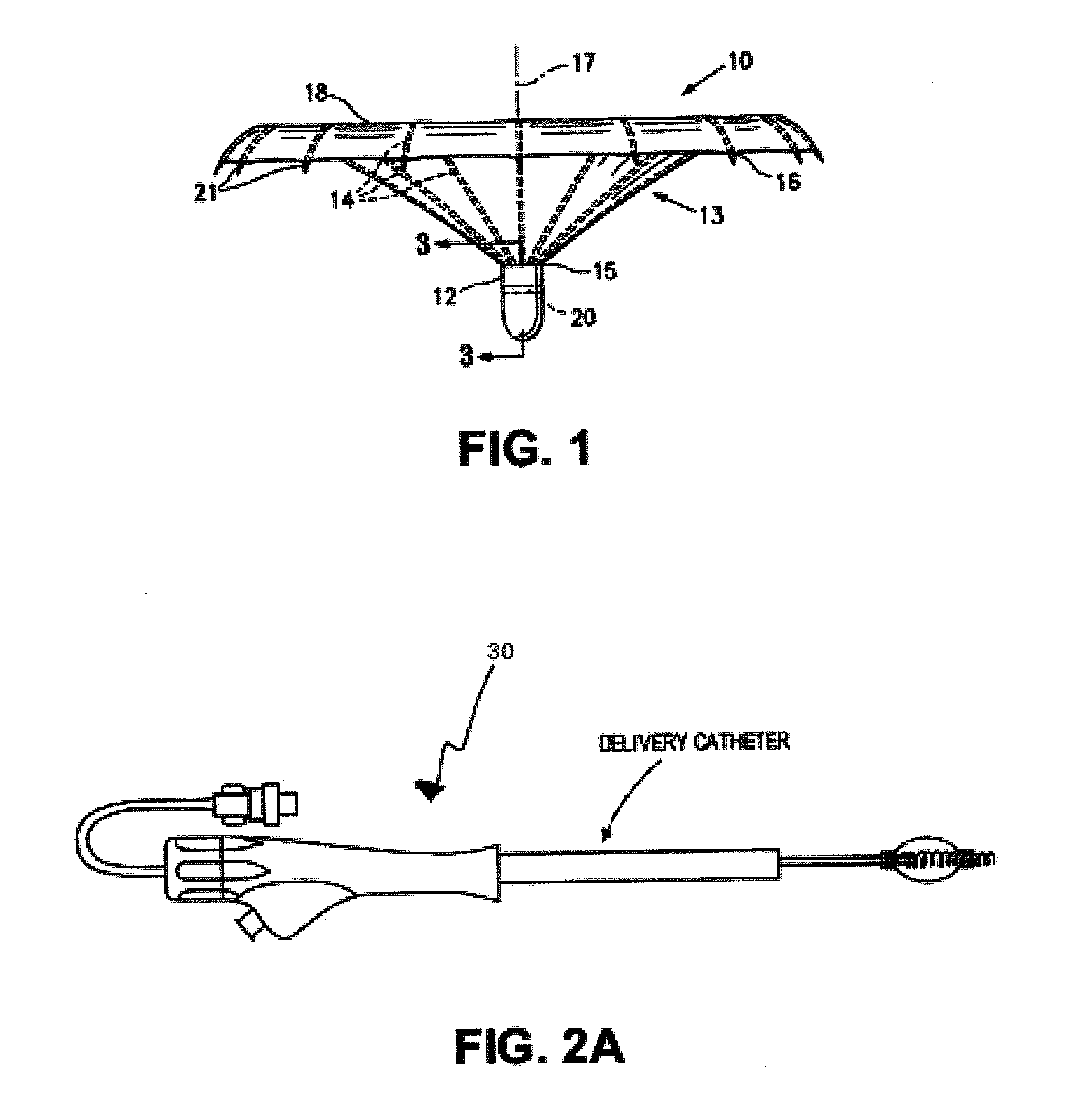
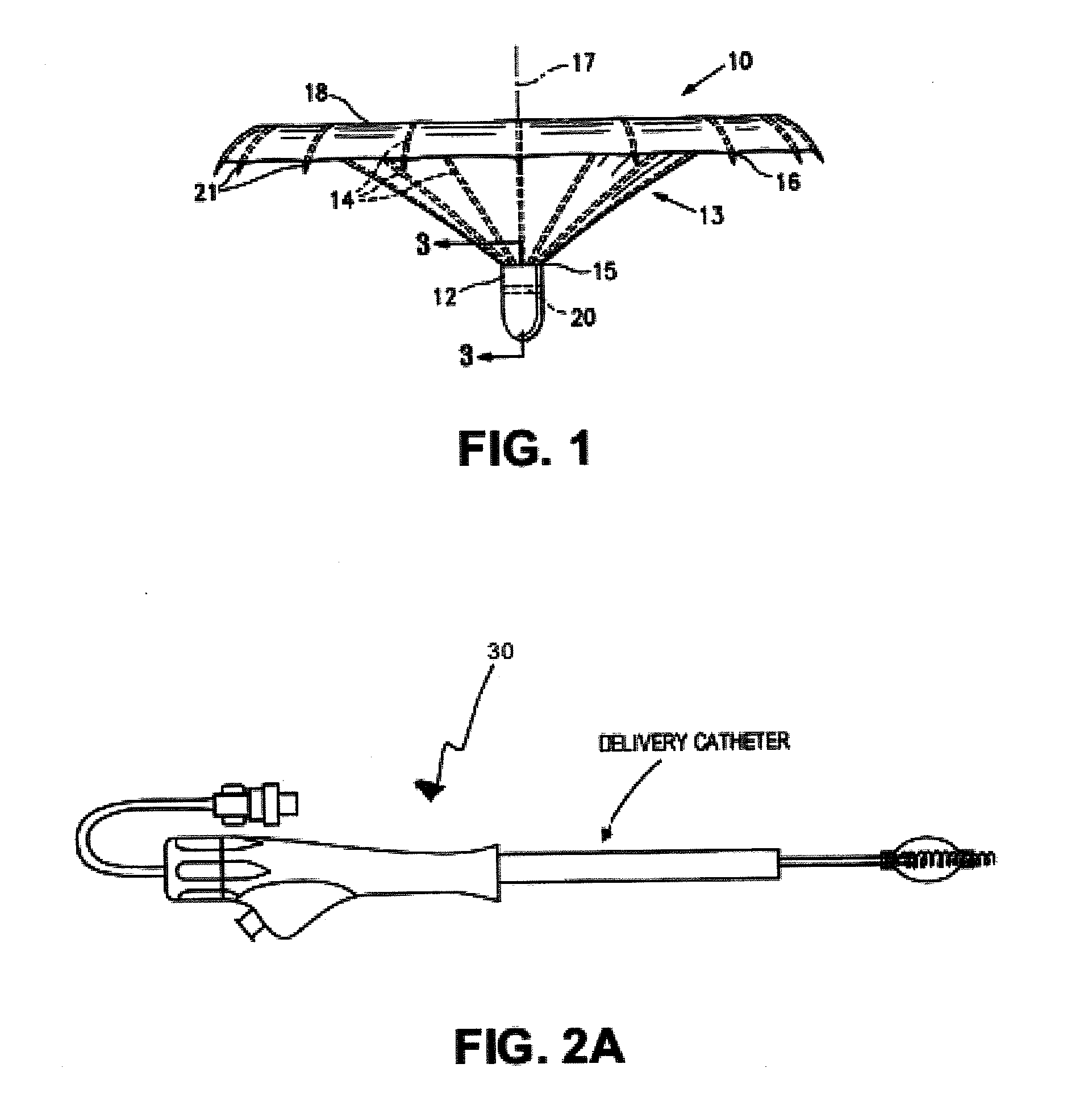
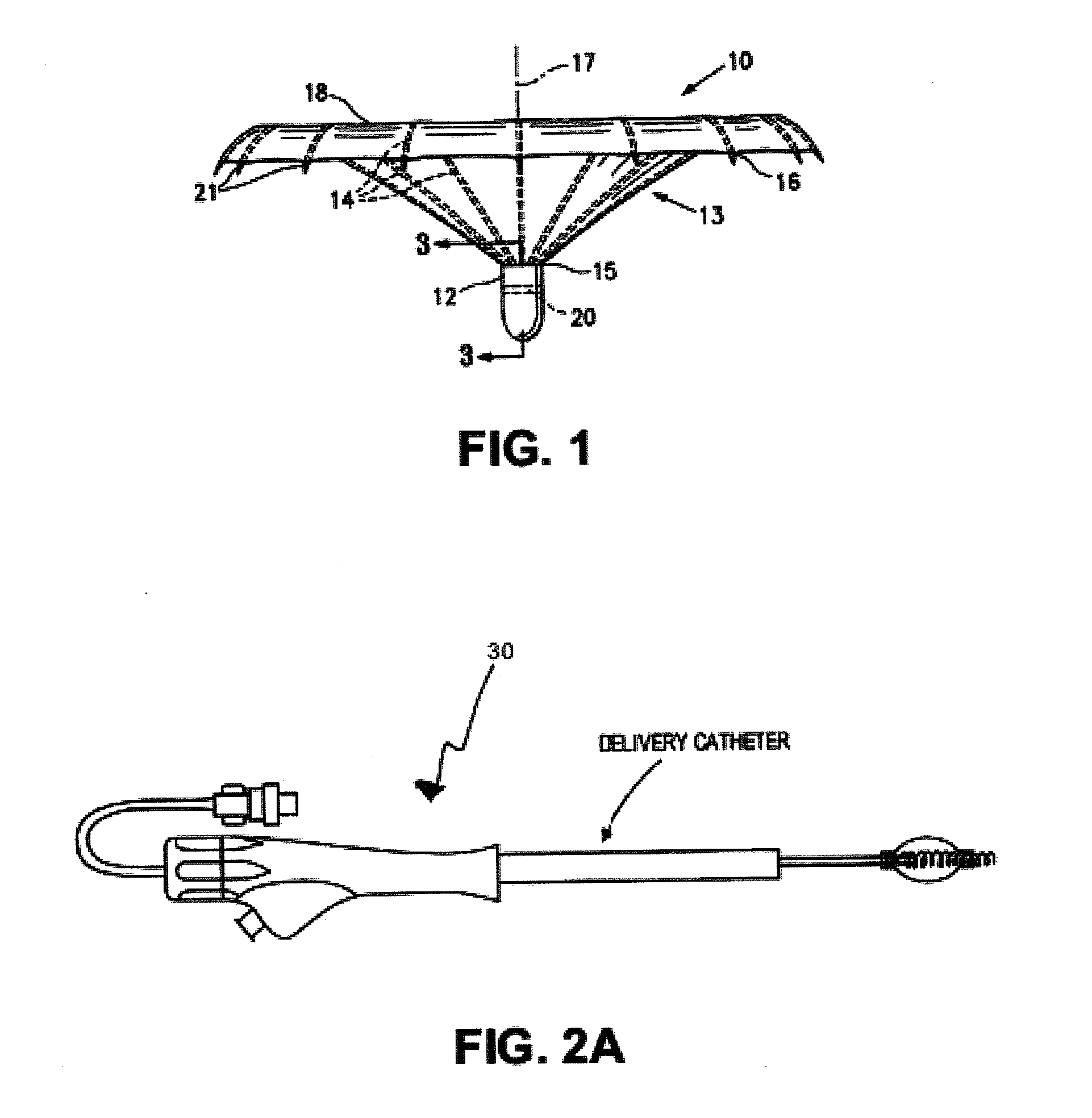
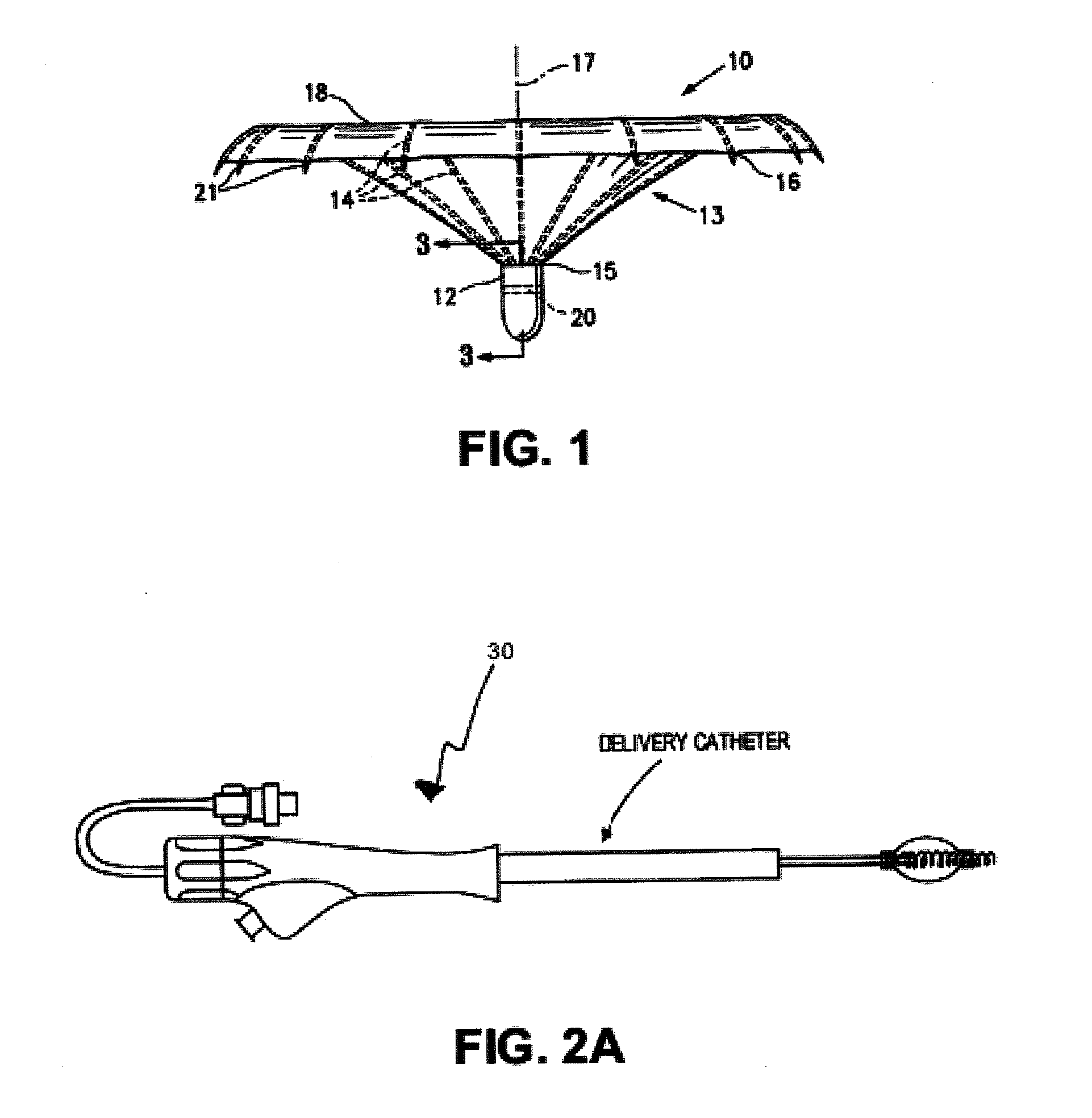
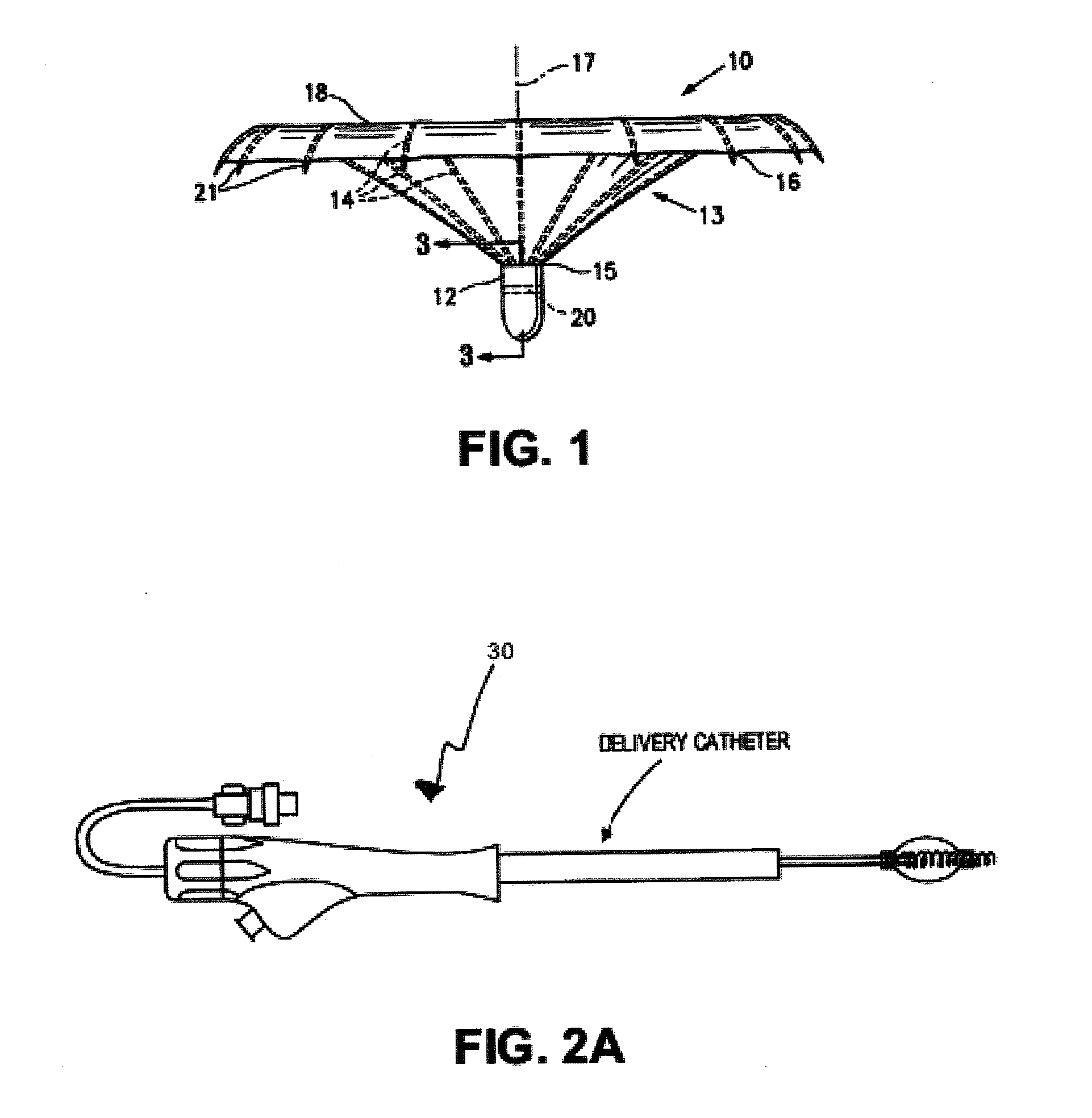
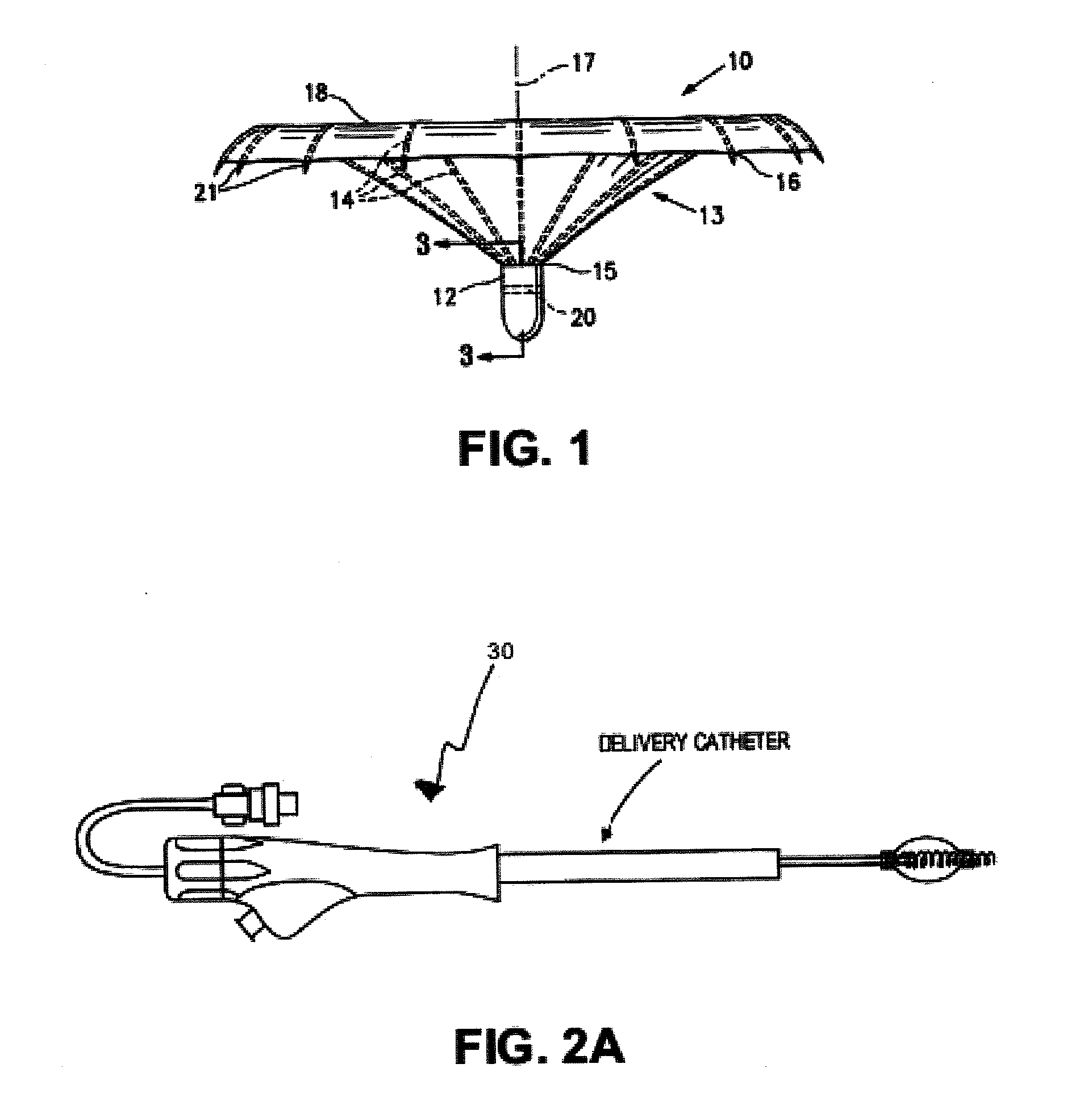
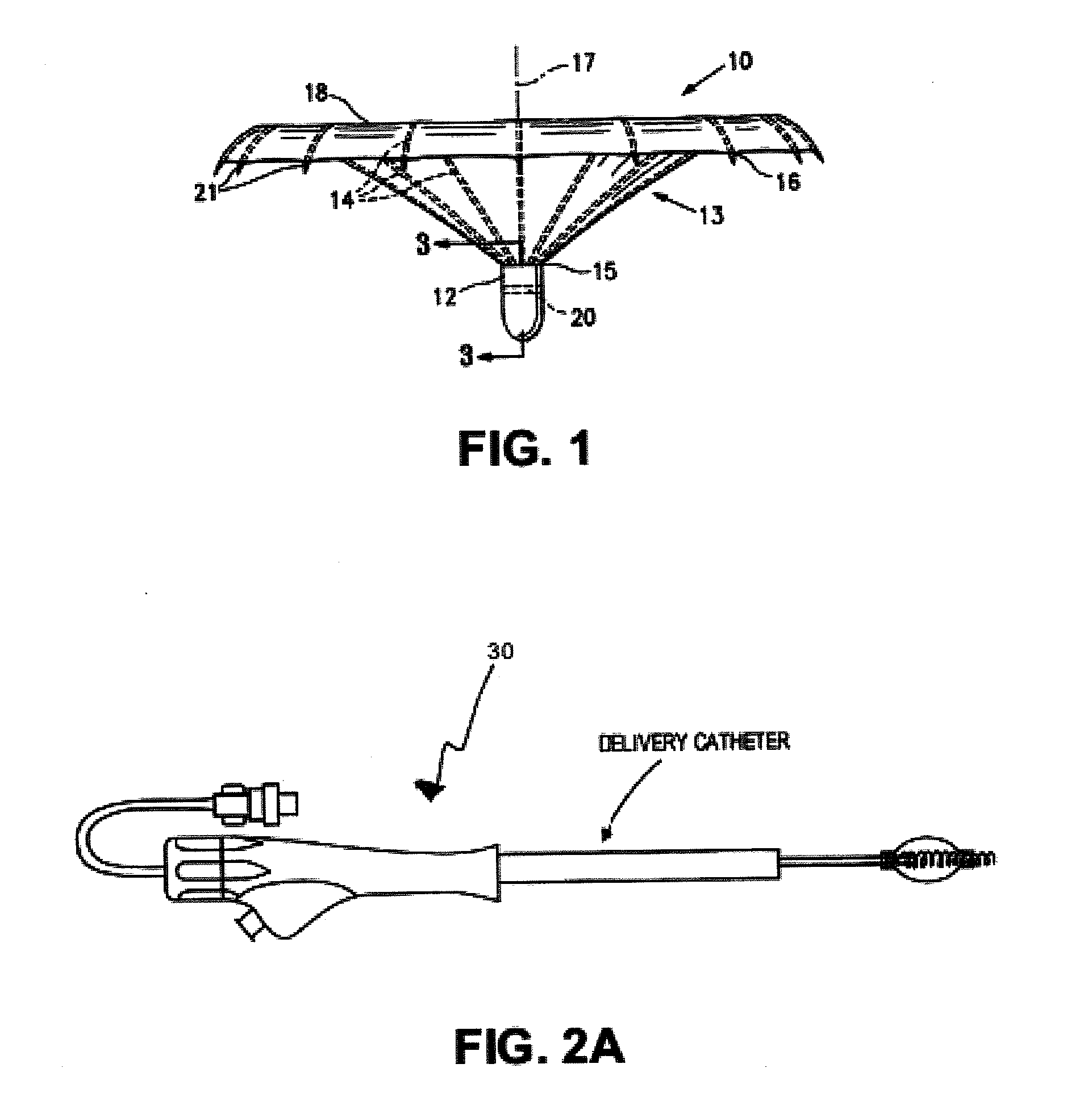
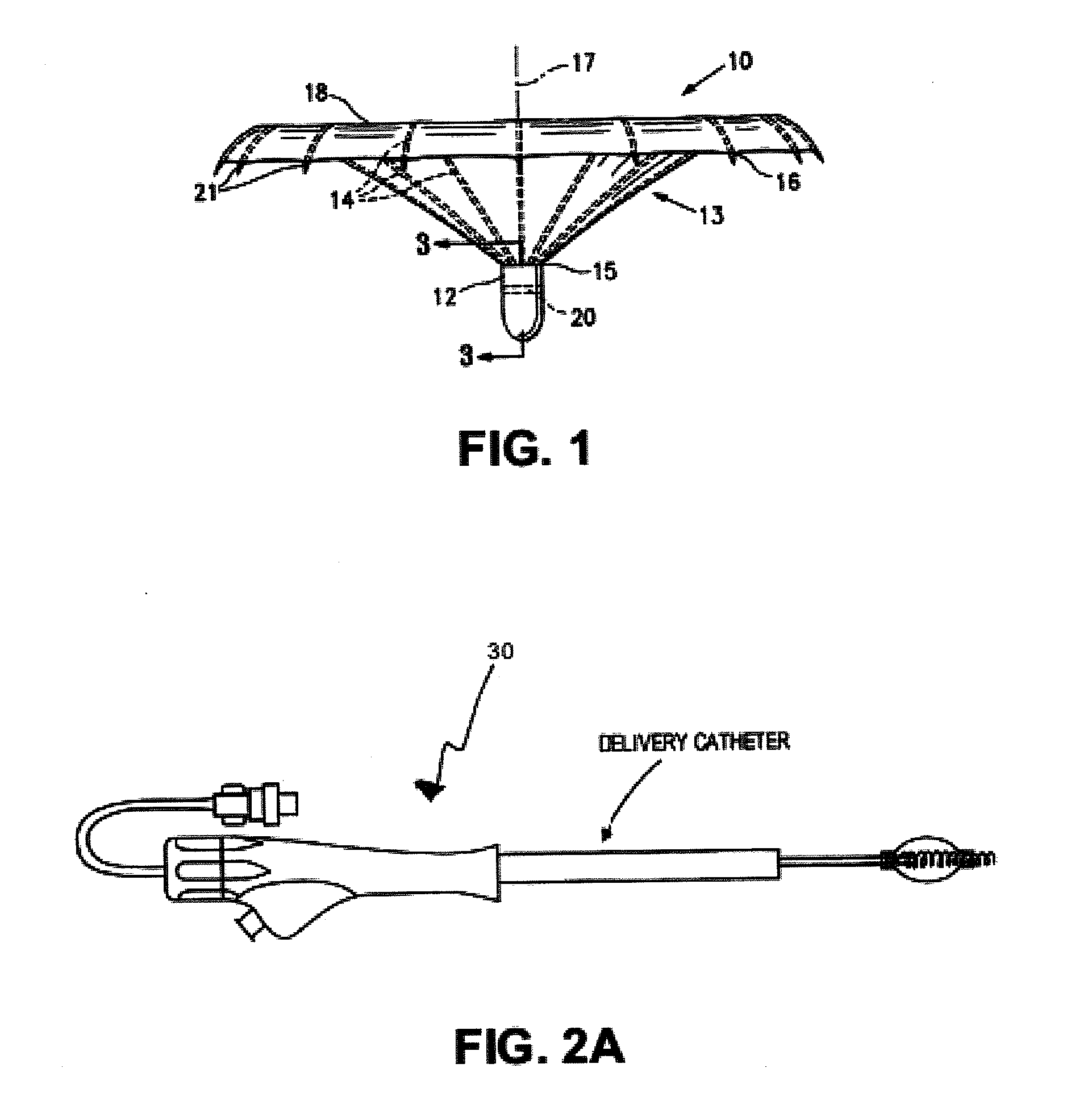
This patent application claims priority as a continuation-in-part of U.S. patent application Ser. No. 12/893,832, filed on Sep. 29, 2010, which is a continuation-in-part of U.S. patent application Ser. No. 11/860,438, filed on Sep. 24, 2007 (which issued as U.S. Pat. No. 7,897,086 on Mar. 1, 2011), which is a continuation-in-part of U.S. patent application Ser. No. 10/913,608, filed on Aug. 5, 2004 (now abandoned). Each of these patent applications is herein incorporated by reference in their entirety. U.S. patent application Ser. No. 12/893,832, filed on Sep. 29, 2010 also claims priority as a continuation-in-part of U.S. patent application Ser. No. 12/509,289, filed on Jul. 24, 2009, which is a continuation of U.S. patent application Ser. No. 11/151,164, filed on Jun. 10, 2005 (which issued as U.S. Pat. No. 7,582,051 on Sep. 1, 2009). U.S. patent application Ser. No. 12/893,832 also claims priority to U.S. provisional patent application Ser. No. 61/246,920, filed Sep. 29, 2009. Each of these patent applications is herein incorporated by reference in their entirety. All publications and patent applications mentioned in this specification are herein incorporated by reference in their entirety, as if each individual publication or patent application was specifically and individually indicated to be incorporated by reference in its entirety. The present invention relates generally to medical/surgical devices and methods pertaining to treating heart disease, particularly heart failure. More specifically, the present invention relates to devices and methods for delivering a partitioning device to a patient's ventricle. Described herein are systems, methods and devices for improving cardiac function, and may relate generally to treating heart disease, particularly heart failure, and more specifically, to systems, methods, and devices for delivering a partitioning device to a patient's ventricle. Heart failure annually leads to millions of hospital visits internationally. Heart failure (including congestive heart failure) is the description given to a myriad of symptoms that can be the result of the heart's inability to meet the body's demand for blood flow. In certain pathological conditions, the ventricles of the heart become ineffective in pumping the blood, causing a back-up of pressure in the vascular system behind the ventricle. The reduced effectiveness of the heart is usually due to an enlargement of the heart. A myocardial ischemia may, for example, cause a portion of a myocardium of the heart to lose its ability to contract. Prolonged ischemia can lead to infarction of a portion of the myocardium (heart muscle) wherein the heart muscle dies and becomes scar tissue. Once this tissue dies, it no longer functions as a muscle and cannot contribute to the pumping action of the heart. When the heart tissue is no longer pumping effectively, that portion of the myocardium is said to be hypokinetic, meaning that it is less contractile than the uncompromised myocardial tissue. As this situation worsens, the local area of compromised myocardium may in fact bulge out as the heart contracts, further decreasing the heart's ability to move blood forward. When local wall motion moves in this way, it is said to be dyskinetic, or akinetic. The dyskinetic portion of the myocardium may stretch and eventually form an aneurysmic bulge. Certain diseases may cause a global dilated myopathy, i.e., a general enlargement of the heart when this situation continues for an extended period of time. As the heart begins to fail, diastolic pressures increase, which stretches the ventricular chamber prior to contraction and greatly increases the pressure in the heart. In response, the heart tissue reforms to accommodate the chronically increased filling pressures, further increasing the work that the now compromised myocardium must perform. Drug therapy typically treats the symptoms of the disease and may slow the progression of the disease, but it cannot cure the disease. One of the only permanent treatments for heart failure is heart transplantation, but heart transplant procedures are very risky, extremely invasive and expensive and are performed on only a small percentage of patients. Many patient's do not qualify for heart transplant for failure to meet any one of a number of qualifying criteria, and, furthermore, there are not enough hearts available for transplant to meet the needs of HF patients who do qualify. Substantial effort has been made to find alternative treatments for heart failure. For example, surgical procedures have been developed to dissect and remove weakened portions of the ventricular wall in order to reduce heart volume. This procedure is highly invasive, risky and expensive and is commonly only done in conjunction with other procedures (such as heart valve replacement or coronary artery by-pass graft). Additionally, the surgical treatment is usually only offered to the most severe class of patients and, accordingly, is not an option for most patients facing ineffective drug treatment. Finally, if the procedure fails, emergency heart transplant is the only presently available option. Ventricular partitioning devices offer a solution for treating heart failure. These devices generally function to partition a patient's ventricle into a productive region and a non-productive region. For such devices to function properly, they are positioned in a specific location within the patient's heart chamber. Delivery of a partitioning device may be made complicated by the anatomy of a patient and by aspects or characteristics of the delivery device or partitioning device itself. Thus, it would be beneficial to provide devices, systems and methods for delivering and deploying a partitioning device in a patient's ventricle. The systems for reducing ventricular volume described herein may include delivery systems and devices for delivering partitioning devices. A partitioning device, or implant, may be an umbrella-shaped partitioning implant, and may be included as part of the system for reducing ventricular volume. The delivery systems may include a guide catheter for guiding the implant to the ventricle, positioning it within the implant, expanding the implant to partition the ventricle, and release the implant from the catheter, deploying it in position. Described herein are systems, apparatus and methods for partitioning a heart. The systems may include a partitioning device or implant, applicators for inserting, repositioning and/or removing them, and methods of positioning, deploying and removing them. The implants described herein are cardiac implants that may be inserted into a chamber of a patient's heart, particularly the left ventricle. The implant may support the heart wall, or in some variations the implant is a ventricular partitioning device for partitioning the ventricle into productive and non-productive regions, and/or for reducing the volume of the ventricle. For example, the devices and systems described herein may include a delivery system (or insertion tools, such as a catheter and sheath/guide tool) and a ventricular partitioning device including a plurality of ribs, configured to expand within the patient's ventricle. The delivery system may include one or more catheters (e.g., a guide catheter, delivery catheter, etc.). In some embodiments, the systems described herein include an elongate catheter having an expandable member at the distal end of the guide catheter configured to expand the ventricular partitioning device and a coupling element at the distal tip of the guide catheter configured to couple the ventricular partitioning device to the guide catheter. Described herein are systems for reducing the volume of a patent's ventricle. The system may include a delivery device (or delivery system) as described in detail herein, as well as a ventricular partitioning device. Any combination of any of the delivery systems and partitioning devices described herein may be used. For example, a system for delivering a ventricular partitioning device into a patient's ventricle and deploying the partitioning device to reduce the effective volume of the ventricle by expanding the partitioning device from a collapsed delivery configuration into an expanded deployed configuration, may include: an elongate guide catheter having a proximal end and a distal end; an expansion member near the distal end of the guide catheter and configured to expand a plurality of struts of the partitioning device by applying pressure to the collapsed partitioning device to open the partitioning device and secure it in the ventricle; and a coupling element distal to the expansion member and configured to deployably secure to a hub of the partitioning device to retain the expansion member at least partially surrounded by the collapsed partitioning device prior to deployment. The system may further comprise an expansion control for expanding the expansion member to apply pressure and expand the ventricular partitioning device. Any appropriate expansion control may be used, including an inflation lumen connected to the expansion member, a pullwire for pulling on the expansion member to expand it, or the like. The expansion control may also include a manipulatable control, such as a button, knob, slider, or dial on the proximal end of the elongate guide catheter for controlling expansion of the expansion member. The system may also include a deployment control for releasing the coupling element from the hub of the ventricular partitioning device. Any appropriate deployment control may be used, including (but not limited to) a torque shaft connected to the coupling element for unscrewing the coupling element from the ventricular partitioning device, a pullwire connected to the coupling element for pulling a hitch pin to release the ventricular partitioning device, or the like. The deployment control and the expansion control may be separately activated. In some variations, the expansion control may be repeatedly activated to expand/contract the partitioning device. As mentioned, any of the systems described herein may also include a ventricular partitioning device. For example, a system may include a ventricular partitioning device comprising an umbrella-like structure having a plurality of struts joined at a central hub. The catheter (e.g., guide catheter) may include any appropriate expansion member. For example, the expansion member may be a hydraulic expansion member comprising a plurality of openings for releasing pressurized fluid to apply pressure to expand the ventricular partitioning device, an inflatable expansion member (e.g., a balloon), or a mechanical expander. A mechanical expansion member may include a plurality of struts joined at their proximal and distal ends and configured to expand outwards when the proximal and distal ends are brought closer together. The catheter may also include any appropriate coupling element, including mechanical coupling members such as helical screws, hitch pins, or the like. In some variations of the system, the guide catheter further comprises a proximal handle having a one-handed activation release. The systems described herein may also include a steering mechanism that bends the distal end region of the guide catheter. The steering mechanism may include tendons or pull wires that pull one or more sides of the catheter to bend the catheter for steering. In some variations, described in greater detail below, the catheter is adapted to be steered by bending selectively in one or more directions. In some variations, the catheter includes hinge-points or cut-out regions that allow for column strength (allowing pushing/pulling of the catheter axially), while making the catheter flexible in one or more directions. The catheter may also be formed of multiple layers; for example, a guide catheter may include an outer catheter formed of a metal or other appropriate material providing column strength and having a lumen in which an inner catheter resides. The inner catheter may also include one or more lumen (e.g., an inflation lumen, a perfusion lumen, etc.). The catheter may also include a pullwire and/or a torque wire. In one variation, a system for delivering a ventricular partitioning device into a patient's ventricle and deploying the partitioning device to reduce the effective volume of the ventricle by expanding the partitioning device from a collapsed delivery configuration into an expanded deployed configuration may include: an elongate guide catheter having a proximal end and a distal end; an expansion member near the distal end of the guide catheter and configured to expand the partitioning device by applying pressure to open the collapsed partitioning device and secure it in the ventricle; a coupling element distal to the expansion member and configured to deployably secure to a hub of the partitioning device to retain the expansion member at least partially surrounded by the collapsed partitioning device prior to deployment; an expansion control at the proximal end of the elongate guide catheter for expanding the expansion member to apply pressure and expand the partitioning device; and a deployment control for releasing the partitioning device from the guide catheter by separating the coupling element from the hub of the partitioning device. As mentioned above, any of the systems described herein, including the system for delivery a partitioning device into a patient's ventricle and deploying the partitioning device, may include any of the features described. For example, the system may include an expansion control comprising an inflation lumen connected to the expansion member a pullwire for pulling on the expansion member to expand it, etc. The system may also include controls such as a button, knob, slider, or dial on the proximal end of the elongate guide catheter for controlling expansion of the expansion member. Also described herein are delivery systems for delivering an umbrella-shaped ventricular partitioning device into a patient's ventricle and mechanically deploying the partitioning device to reduce the effective volume of the ventricle by expanding the partitioning device from a collapsed configuration into an expanded configuration. These systems may comprise: an elongate guide catheter having a proximal end and a distal end; a mechanical expander near the distal end of the guide catheter having a plurality of arms configured to extend outwards when operated to apply pressure to the partitioning device to open the partitioning device; and a coupling element distal to the expansion member and configured to deployably secure to a central hub of the partitioning device and to retain the expansion member at least partially surrounded by the collapsed partitioning device prior to deployment. Also described herein are delivery system for delivering an umbrella-shaped ventricular partitioning device into a patient's ventricle and deploying the partitioning device to reduce the effective volume of the ventricle by expanding the partitioning device from a collapsed configuration into an expanded configuration, the system comprising: an elongate guide catheter having a proximal end and a distal end; a mechanical expander near the distal end of the guide catheter comprising a plurality of arms joined at their proximal and distal ends and configured to expand outwards when the proximal and distal ends are brought closer together, the mechanical expander configured to apply pressure the partitioning device to open the partitioning device and secure it in the ventricle; and a coupling element distal to the expansion member and configured to deployably secure to a hub of the partitioning device and to retain the expansion member at least partially surrounded by the collapsed partitioning device prior to deployment. In some variations, a delivery system for delivering an umbrella-shaped ventricular partitioning device into a patient's ventricle and deploying the partitioning device to reduce the effective volume of the ventricle by expanding the partitioning device from a collapsed configuration into an expanded configuration, includes: an elongate guide catheter having a proximal end and a distal end; an inflatable expander near the distal end of the guide catheter configured to extend outwards when inflated to apply pressure to open the partitioning device and to secure the partitioning device in the ventricle; a distal nose spacer distal to the inflatable expander on the guide catheter and configured to space the inflatable expander proximally from a central hub region of the partitioning device; a taper region between the distal nose spacer and the inflatable expander; and a coupling element distal to the expansion member and configured to deployably secure to the central hub of the partitioning device and to retain the expansion member at least partially surrounded by the partitioning device prior to deployment. Also described herein are delivery systems for delivering an umbrella-shaped ventricular partitioning device into a patient's ventricle and mechanically deploying the partitioning device to reduce the effective volume of the ventricle by expanding the partitioning device from a collapsed configuration into an expanded configuration, the system comprising: an elongate guide catheter having a proximal end and a distal end; a pressure expander near the distal end of the guide catheter comprising a plurality of openings from a fluid source line extending along the length of the elongate catheter, the plurality of openings positioned near the distal end region of the elongate guide catheter and configured to release fluid and apply pressure to the proximal end region of the partitioning device to expand the partitioning device; and a coupling element distal to the expansion member and configured to deployably secure to a central hub of the partitioning device and to retain the expansion member at least partially surrounded by the partitioning device prior to deployment. Also described are systems for reducing the effective volume of the ventricle by securing a ventricular partitioning device within the ventricle, the system comprising: an umbrella-shaped ventricular partitioning device having a central hub, a plurality of struts, and a membrane, wherein the partitioning device has a collapsed delivery configuration and an expanded deployed configuration; and a delivery system. The delivery system may include: an elongate guide catheter having a proximal end and a distal end; a mechanical expander near the distal end of the guide catheter comprising a plurality of arms joined configured to extend outwards to expand the ventricular partitioning device by applying pressure against the struts to open the ventricular partitioning device; a expansion pullwire coupled to the mechanical expander; and a coupling element distal to the expansion member and configured to deployably secure to the central hub of the partitioning device and to retain the expansion member at least partially surrounded by the collapsed partitioning device prior to deployment. Methods of partitioning a ventricle, and method of reducing ventricular volume, are also described. The methods described herein may generally include the steps of advancing the distal end of a delivery or guide catheter into the patient's ventricle, positioning the distal end of the guide catheter within the ventricle, expanding a ventricular partitioning device within the ventricle to partition the ventricle, and deploying the ventricular partitioning device from the distal end of the guide catheter. The device may be secured, and/or sealed, to the ventricle wall(s). For example, described herein are methods of reducing ventricular volume to treat heart disease, the method comprising: positioning an umbrella-shaped, expandable partitioning device having a reinforced membrane in a contracted configuration near the apex of a patients' ventricle using an elongate guide catheter to which the partitioning device is releasably coupled; expanding an expansion member near the distal end of the guide catheter to apply pressure to the proximal end region of the contracted partitioning device to expand the partitioning device; and releasing a coupling element distal to the expansion member on the guide catheter to deploy the partitioning device. In some variations, the method also includes a step of securing the periphery of the partitioning device to the ventricle wall. For example, the guide catheter may be configured to expand to drive open the partitioning device and secure it to the wall of the ventricle. The method may also include the step of sealing the periphery of the partitioning device to the ventricle wall. In some variations, the method also includes percutaneously guiding the partitioning device on the end of the guide catheter into the ventricle. For example, the method may include advancing the partitioning device into the ventricle through an inner lumen of a delivery catheter. The method may include the step of expanding the expansion member by expanding an inflatable expansion member near the distal end of the guide catheter. The step of expanding the expansion member may comprise expanding a plurality of arms joined at their proximal and distal ends by expand bringing the proximal and distal ends closer together. In some variations, the step of expanding the expansion member comprises expelling fluid from a plurality of openings positioned near the distal end region of the guide catheter to apply pressure to the proximal end region of the partitioning device to expand the partitioning device. The step of releasing a partitioning device from the catheter (guide catheter that has guided and positioned the device) may be preformed after the device has been positioned in the appropriate region of the ventricle, typically the apical region. This guidance may be performed under visualization, such as fluoroscopy. Once positioned, the device may be deployed and released from the catheter by disengaging the coupling member. For example, the coupling element may be released by rotating a torque shaft that rotates to withdraw a helical coil screw (e.g., the screw and torque shaft may form part of the coupling element) from a hub of the partitioning device. Also described are delivery systems for transvascular delivery of a ventricular partitioning device into a patient's ventricle and deploying the partitioning device to reduce the effective volume of the ventricle by expanding the partitioning device from a collapsed delivery configuration into an expanded deployed configuration. In general, the delivery systems may include an elongate guide catheter having a proximal end and a distal end; a conical dilator at the distal end of the elongate guide catheter, the conical dilator being removable to enable delivery of the ventricular partitioning device; a delivery catheter having a proximal end and a distal end; an expansion member near the distal end of the delivery catheter and configured to expand a plurality of struts of the partitioning device by applying pressure to the collapsed partitioning device to open the partitioning device and secure it in the ventricle; a coupling element configured to deployably secure to a hub of the partitioning device to retain the expansion member at least partially surrounded by the collapsed partitioning device prior to deployment. In some embodiments, the expansion member is an inflatable balloon. In some embodiments, the coupling element comprises a helical screw. In some embodiments, the delivery system may further include a ventricular partitioning device wherein the ventricular partitioning device comprises an umbrella-like structure having a plurality of struts joined at a central hub. In some embodiments, the central hub is coupled to the coupling element such that the central hub is distal to plurality of struts. In some embodiments, the partitioning device has a central axis of symmetry. In some embodiments, the partitioning device has an asymmetric configuration around the hub. In some embodiments, the delivery system may further include a steering mechanism that bends the distal end region of the guide catheter. In some embodiments, the delivery catheter is steerable. In some embodiments, the delivery system may further include at least one radio-opaque marker. In some embodiments, the delivery system may further include a guidewire lumen. In some embodiments, the guidewire lumen is continuous through the length of the delivery system. In some embodiments, the guidewire lumen is configured as a rapid-exchange feature. In some embodiments, the delivery system may further include a guidewire. In some embodiments, the guidewire includes a distal tip with an anchoring mechanism for anchoring to a cardiac wall. Also described herein are methods for reducing ventricular volume to treat heart disease. In general the methods may include the steps of positioning an umbrella-shaped, expandable partitioning device having a reinforced membrane in a contracted configuration near the apex of a patients' ventricle using an elongate delivery catheter to which the partitioning device is releasably coupled; expanding an expansion member near the distal end of the delivery catheter to apply pressure to the proximal end region of the contracted partitioning device to expand the partitioning device; and releasing a coupling element distal to the expansion member on the delivery catheter to deploy the partitioning device. In some embodiments, the methods may further include the step of securing the periphery of the partitioning device to the ventricle wall. In some embodiments, the methods may further include the step percutaneously delivering the partitioning device on the end of the delivery catheter into the ventricle. In some embodiments, the methods may further include the step advancing the partitioning device into the ventricle through an inner lumen of a delivery catheter. In some embodiments, the step of expanding the expansion member comprises expanding an inflatable expansion member near the distal end of the delivery catheter. In some embodiments, the step of releasing comprises rotating a torque shaft to withdraw a helical coil screw from a hub of the partitioning device. In some embodiments, the methods may further include the step of positioning the delivery system using a guidewire. In some embodiments, the step of positioning the delivery system using a guidewire further comprises positioning the delivery system over a guidewire. In some embodiments, the guidewire is anchored to an intended landing zone on the patient's ventricle. In some embodiments, the patient's ventricle is obtained using a vascular conduit as an access route. In some embodiments, the vascular conduit is part of an arterial circulation. In some embodiments, the vascular conduit is part of a venous circulation, and the access route comprises a transseptal passage. In some embodiments, the transseptal passage is an inter-atrial passage through a foramen ovale. Also described herein are delivery systems for transapical delivery of a ventricular partitioning device into a patient's ventricle and deploying the partitioning device to reduce the effective volume of the ventricle by expanding the partitioning device from a collapsed delivery configuration into an expanded deployed configuration. In general the systems include an elongate access sheath having a proximal end and a distal end; an elongate delivery catheter having a proximal and distal end; an expansion member near the distal end of the delivery catheter and configured to expand a plurality of struts of the partitioning device by applying pressure to the collapsed partitioning device to open the partitioning device and secure it in the ventricle; and a coupling element proximal to the expansion member and configured to deployably secure to a hub of the partitioning device to retain the expansion member at least partially surrounded by the collapsed partitioning device prior to deployment. In some embodiments, the partitioning device has a central axis of symmetry; while in some embodiments, the partitioning device has an asymmetric configuration around the hub. In some embodiments, the elongate delivery catheter is a delivery shaft. In some embodiments, the delivery shaft is rigid. In some embodiments, the delivery system further includes a ventricular partitioning device wherein the ventricular partitioning device comprises an umbrella-like structure having a plurality of struts joined at a central hub. In some embodiments, the central hub is coupled to the elongate delivery catheter such that the central hub is proximal to plurality of struts. In some embodiments, the expansion member is an inflatable balloon. In some embodiments, the coupling element comprises a helical screw. Also described herein is a transapical method of reducing ventricular volume to treat heart disease. In general, the method may include the steps of positioning an umbrella-shaped, expandable partitioning device having a reinforced membrane in a contracted configuration near the apex of a patient's ventricle using an elongate access sheath to which the partitioning device is releasably coupled; expanding an expansion member to apply pressure to the proximal end region of the contracted partitioning device to expand the partitioning device; and releasing a coupling element proximal to the expansion member to deploy the partitioning device. In some embodiments, the positioning step further comprises accessing the patient's ventricle through the apex of the patient's heart. In some embodiments, the method may further include the step of creating a cardiotomy near the apex of the patient's heart. In some embodiments, the method may further include the step of accessing the patient's heart through an intercostal access route. In some embodiments, the accessing step further comprises accessing the patient's heart percutaneously, while in some embodiments, the accessing step further comprises accessing the patient's heart surgically. In some embodiments, the method may further include the step of pulling a delivery sheath in the proximal direction to release the partitioning device. In some embodiments, the method may further include the step of pushing a delivery sheath in the distal direction over the partitioning device to collapse the partitioning device for removal or redeployment. Devices, systems and methods for reducing ventricular volume by partitioning the ventricle may be used to treat cardiac or circulatory disorders. In general, the devices and systems described herein include partitioning devices for partitioning the ventricle into productive and non-productive regions. The partitioning device described herein may also be referred to as a ventricular volume reduction devices or implants. Also described herein are delivery devices for delivering and/or deploying the ventricular volume reduction implants. The delivery devices may also be referred to as catheters, or more specifically as guide catheters. As used herein, a guide catheter may be used for delivering and/or deploying a partitioning device into a patient's ventricle. Any of the systems described herein may include both a guide catheter and a partitioning device/volume reduction device. A partitioning device may be pre-loaded onto the guide catheter. The following description is not intended to limit the invention to the illustrated embodiments, but rather to enable any person skilled in the art to make and use this invention. A ventricular partitioning device typically includes a plurality of ribs, configured to expand within the patient's ventricle, and a membrane that may be reinforced by the ribs. The ribs may also be referred to as struts. In some variations, the partitioning device/volume reduction device may be an umbrella-type device or implant, having a hub to which the ribs or struts extend; the device may have a collapsed delivery configuration (resembling a collapsed umbrella) and an expanded delivery configuration. Although the partitioning device may be pre-biased in the expanded configuration, the delivery device (guide catheter) may include an expansion element to help fully expand, position, and secure the implant in the ventricle. For example, in some variations the implant includes a plurality of struts or ribs formed of a memory material such as Nitinol that self-expands at least partially into the deployed configuration. When deploying with a guide catheter, the guide catheter may force expansion of the partitioning device and insertion into the wall of the ventricle. In some examples, the systems described herein include an elongate guide catheter having an expandable member at the distal end of the guide catheter configured to expand the ventricular partitioning device and a coupling element at the distal tip of the guide catheter configured to couple the ventricular partitioning device to the guide catheter. In general, the methods described herein include the steps of advancing the distal end of a guide catheter into the patient's ventricle, positioning the distal end of the guide catheter within the ventricle, deploying the ventricular partitioning device from the distal end of the guide catheter, and expanding a ventricular partitioning device within the ventricle to partition the ventricle. The guide catheter has an inner lumen 33 extending between the proximal end 34 and distal end 35. A haemostatic valve (not shown) may be provided at the proximal end 34 of the guide catheter 31. A flush port 36 on the proximal end 34 of guide catheter 31 is in fluid communication with the inner lumen 33. The delivery catheter 32 has an outer shaft 40 with an inner lumen 41 and a proximal injection port 42, an inner shaft 43 disposed within the inner lumen 41 with a first lumen 44 and a second lumen 45. Balloon inflation port 46 is in fluid communication with the first lumen 44 and flush port 47 is in fluid communication with the second lumen 45. Torque shaft 48 is rotatably disposed within the second lumen 44 of the inner shaft 43 and has an injection port 49 provided at its proximal end 50 in fluid communication with the inner lumen 51 of the torque shaft. The torque shaft 48 in this example is formed at least in part of a hypotube formed of suitable material such as superelastic Nitinol or stainless steel. A torque knob 52 is secured to the proximal end 50 of torque shaft 48 distal to the injection port 49. A helical coil screw 53 is secured to the distal end 54 of the torque shaft 48 and rotation of the torque knob 52 on the proximal end 50 of the torque shaft 48 rotates the screw 53 on the distal end 54 of torque shaft 48 to facilitate deployment of a partitioning device 10. In this example, the screw and torque shaft form a coupling element on the guide catheter that may releasably secure a partitioning device so that it may be delivered. An inflatable balloon 55 is sealingly secured to the distal end of the inner shaft 43 and has an interior 56 in fluid communication with the first lumen 44. The inflatable expansion member is but one variation of an expansion member that may form part of the guide catheter. Inflation fluid may be delivered to the interior 56 through port 44 As mentioned, to deliver the partitioning component 10, it is secured to the distal end of the delivery catheter 32 by means of a coupling mechanism, such as a helical coil screw. The partitioning component 10 is collapsed to a first, delivery configuration which has small enough transverse dimensions to be slidably advanced through the guide catheter 31 ( The partitioning component 10 mounted on the coupling element (screw 53, as shown) may be urged partially out of the inner lumen of the guide catheter 31 until the hub 12 engages the heart wall as shown in With the partitioning component deployed within the heart chamber and preferably partially secured therein, inflation fluid may be introduced through the inflation port 46 into first lumen 44 of inner shaft 43 of the delivery catheter 32 where it is directed through port 44 With the partitioning device 10 properly positioned within the heart chamber, the knob 52 on the torque shaft 48 is rotated counter-clockwise to disengage the helical coil screw 53 of the delivery catheter 32 from the hub 12. This is illustrated in The proximal end of the guide catheter 31 may be provided with a flush port 36 to inject therapeutic or diagnostic fluids through the inner lumen 33. Similarly, the proximal end of the delivery catheter 32 may be provided with a flush port 42 in communication with inner lumen 41 for essentially the same purpose. An inflation port 46 is provided on the proximal portion of the delivery catheter for delivery of inflation fluid through the first inner lumen 44 to the interior 56 of the balloon 55. Flush port 47 is provided in fluid communication with the second inner lumen 45 of the inner shaft 43. An injection port 49 may be provided on the proximal end of the torque shaft 48 in fluid communication with the inner lumen 51 of the torque shaft for delivery of a variety of fluids. The partitioning component 10 in this example partitions the patient's heart chamber 57 into a main productive or operational portion 58 and a secondary, essentially non-productive portion 59, thereby reducing the ventricular volume. The operational portion 58 is much smaller than the original ventricular chamber 57 and provides for an improved ejection fraction. The partitioning increases the ejection fraction and provides an improvement in blood flow. Over time, the non-productive portion 59 fills first with thrombus and subsequently with cellular growth. Bio-resorbable fillers such as polylactic acid, polyglycolic acid, polycaprolactone and copolymers and blends may be employed to initially fill the non-productive portion 59. Fillers may be suitably supplied in a suitable solvent such as DMSO. Other materials which accelerate tissue growth or thrombus may be deployed in the non-productive portion 59. The delivery system 30 includes a guide catheter 31 and a delivery catheter 32. As in the variation shown in The delivery catheter 32 has an outer shaft 37 with an adapter 38 on the proximal end thereof having a proximal injection port 39 which is in fluid communication with the interior of the shaft 37. The outer shaft 37 may have an inner shaft which is disposed within the interior thereof and is secured to the inner surface of the outer shaft by webs which extend along a substantial length of the inner shaft. The injection port may be in fluid communication with the passageways between the inner and outer shafts and defined in part by the webs. A torque shaft, which is preferably formed of hypotubing (e.g. formed of stainless steel or superelastic NiTi), may be disposed within the inner lumen of the inner shaft and has a proximal end 46 secured within the adapter 38. Balloon inflation port 47 is in fluid communication with the inner lumen of the torque shaft 44. Torque shaft 44 is rotatably disposed within the inner lumen 45 of the inner shaft 41 and is secured to rotating knob 49. A helical coil screw 50 is secured to the distal end 51 of the torque shaft 44 and rotation of the torque knob 49 on the proximal end 46 of the torque shaft 44 rotates the screw 51 to facilitate deployment of a partitioning device 10. The proximal end 52 of inflatable balloon 53 is sealingly secured by adhesive 54) about the torque shaft 44 proximal to the distal end 51 of the torque shaft. The balloon 53 has an interior 55 in fluid communication with the inner lumen 48 of the torque shaft 44. Inflation fluid may be delivered to the balloon interior 55 through port 47 which is in fluid communication with the inner lumen 48 of the torque shaft 44. The distal end 56 of the balloon 53 is sealingly secured by adhesive 57 to the helical screw 50. The proximal and distal ends 52 and 56 of the balloon 53 are blocked by the adhesive masses 54 and 57 to prevent the loss of inflation fluid delivered to the interior 55 of the balloon 53. Delivery of inflation fluid through a fluid discharge port 58 in the distal end 51 of the torque shaft 44 inflates the balloon 53 which in turn applies pressure to the proximal surface of the partitioning device 10 to facilitate securing the partitioning component 10 to the wall 59 of heart chamber. The device may be inserted substantially as shown in In The proximal end 34 of the guide catheter 31 is provided with a flush port 36 to inject fluids such as therapeutic, diagnostic or other fluids through the inner lumen 33 during the procedure. Similarly, the proximal injection port 39 of adapter 38 is in communication with passageways 43 if the delivery catheter 32 for essentially the same purpose. In this example, the implant also includes a sealing element, strand 19, which may be used to help stiffen the edge of the membrane so that it may lie against the ventricle wall and form a seal against the wall. The strand may also be used to help retrieve the device. In some embodiments, as the guide catheter 31 is withdrawn, it begins to bend as it is withdrawn through the vascular anatomy of the patient, through the aortic arch, for example. In some instances, this bend may drive the distal tip of the delivery catheter, and therefore the partitioning device, out of position. For example, the guide catheter may drive the device towards the center of the heart, i.e. towards the ventricular septum. In some instances, it may be preferred that the delivery catheter and/or partitioning device are not moved or repositioned by the guide catheter as it is withdrawn. This may be accomplished in one of several embodiments. In a first embodiment, as shown in In some alternative embodiments, as shown in In another alternative embodiment, not shown, the delivery catheter may be a shape set material, such as Nitinol. In some variations, the delivery catheter may be stiffer than the guide catheter, such that as the guide catheter is retracted or withdrawn, it imparts minimal forces on the more stiff delivery catheter. The delivery catheter may be set into any suitable shape, and be configured for any suitable vascular anatomy. In some variations, the size of the expandable member may be limited by the size of the delivery diameter. For example in the stored configuration, i.e. when the expandable member, partitioning device, and the delivery catheter are within the guide catheter, each of the components contributes to the overall delivery diameter. The delivery diameter is preferably small to enable the passing of the guide catheter through the vasculature of the patient, therefore limiting the size of the expandable member and/or the size of the delivery catheter. To address these restrictions, in some variations (e.g., In one variation, illustrated in As shown in Another example of an expandable member is shown in As shown in As shown in In general, it may be beneficial to have the mechanical expansion member be formed of a shape memory or hyperelastic material such as Nitinol. However, it may be desirable to have the rest of the catheter (e.g., the rest of the body region proximal to the expansion member) formed of a different material, such as stainless steel. In some variations the expandable member is a pneumatic, or fluid-pressure based member, as shown in In general, after a partitioning device 10 has been properly positioned within the ventricle, the partitioning device 10 may be deployed and/or released from the guide catheter. As shown in In one variation, shown in The partitioning device may be coupled to the delivery catheter and then released in one of several embodiments. In some embodiments, a torque shaft within the delivery system is rotated to disengage the helical coil screw 53 of the delivery catheter 32 from the hub 12. The rotation of the torque shaft 48 rotates the helical coil screw 53 which rides on the connector bar 20 secured within the hub 12. Once the helical coil screw 53 disengages the connector bar 20, the delivery system 30, including the guide catheter 31 and the delivery catheter 32, may then be removed from the patient. In alternative embodiments, as shown in As shown in In some embodiments a conical dilator 3400, as illustrated in Once the guide catheter is delivered within the patient's heart, specifically within the left ventricle, the conical dilator may be removed from the guide catheter, prior to introduction of the delivery catheter-implant assembly into the guide catheter and/or prior to the delivery of the implant. In some embodiments, the tapered dilator may be removed by and/or with the guidewire. In some embodiments, as shown in In some embodiments, the guidewire may include an anchoring mechanism at the distal tip of the guidewire, for instance a threaded tip, which may be employed to anchor the wire at the intended anchoring site within the patient's ventricle, thus allowing the wire to act as an anchor for delivery of the partitioning device. For example, the guidewire may be positioned within the ventricle, and the distal tip of the guidewire may then be anchored or otherwise coupled to the ventricular wall. Once the guidewire is in position, the implant may be deployed over the guidewire into the patient's ventricle. In some embodiments of the device, radio-opaque markers may be incorporated into the device. The markers may be included on the implanted partitioning device and/or on the delivery system. Radio-opaque markers may be constructed from biocompatible heavy metals, such as gold, platinum and tantalum, and may be fabricated in any form or shape suitable for the intended device, such as bands, tabs, ribbons, disks and the like. They may be in the form of components specifically included for the purpose of providing radio-opacity, or they may be inherent components of a device, made out of a radio-opaque material to provide radio-opacity. In some embodiments, as shown in In some embodiments the systems and methods described herein may be capable of delivering a partitioning device to a ventricle by a transseptal approach. This approach may advantageously be used in patients with compromised femoral arterial anatomy, with a compromised aorta or aortic valve, and/or where delivery through an arterial approach may be considered undesirable or unfeasible. In a typical transseptal procedure access to the left heart is achieved by way of the right heart, typically the right atrium. Access to the right heart is generally achieved by means of a venous access, for instance through a femoral or jugular vein. A guidewire may be used to establish the access route, and may be threaded through a cardiac septum, for instance through the inter-atrial foramen ovale to establish access to the left heart. Subsequently, the guidewire may be routed through the mitral valve into the left ventricle and to vicinity of the apex of the heart. Alternatively, the use of the guidewire may be limited to access to the left atrium. Passage of a guide catheter through the foramen may be enabled by the use of a conical dilator, as described above in reference to Alternatively, positioning of the delivery catheter may be achieved with a steerable guide catheter and/or delivery catheter, as described above in reference to In some embodiments, as shown in The transapical approach may be advantageously used in patients with extensive vascular or valvular disease, where delivery through a transvascular approach is undesirable or even unfeasible. As shown in As shown in The access sheath or guide catheter may be withdrawn from the cardiotomy 301, allowing the ventricular wall 300 to seal against the delivery shaft 302. In some embodiments the access sheath may be a splittable sheath, to facilitate removal from the cardiotomy and the delivery shaft. The delivery shaft 302 may be moved in a proximal direction (i.e. out of the heart) in the cardiotomy 301, allowing it to pull a central hub 306 of the partitioning device onto the ventricular wall 300. In some embodiments an expansion member, such as a balloon 308 or a mechanical expansion member may be located on the device 303 in a location distal to the device, i.e. in a location facing the ventricular lumen and away from the apex. The expansion member 308 may be expanded to fully deploy and anchor the partitioning device 303. After collapsing or deflating, the expansion device 308 may be withdrawn through the continuous lumens 310 and 311. Alternatively, the expansion device may be removed together with the delivery shaft 302 after passing lumen 311. The delivery 302 shaft may be disconnected from the partitioning device 303 and withdrawn from the cardiotomy 301, and the cardiotomy 301 may be closed in a standard manner, for instance with a purse-string suture. In some alternative embodiments of a percutaneous transapical method of delivery of the device 303, access may be achieved by direct puncture of the ventricular wall 300 at the transapical access zone 204 with a micropuncture needle, followed by advancing a guidewire (not shown) through the needle and exchanging the needle for an appropriate access sheath or a specifically designed guide catheter. Deployment of the device 303 and retrieval of the delivery shaft 302 may be similar or identical to the procedures used after surgical access. Closure of the cardiotomy 301 may be achieved with a percutaneous closure device. During transapical access, the central hub of the partitioning device may be located co-axially with the cardiotomy. However, the cardiotomy may not be located centrally to the segment of the ventricular wall to be partitioned away from the lumen of the ventricle. Therefore, in some cases, the use of a partitioning device with an axis of symmetry at a central hub may not result in optimal coverage of an ineffective segment of the ventricular wall. In such cases, use of an asymmetric partitioning device, as illustrated in In some embodiments, as shown in In some embodiments of the device, radio-opaque markers may be incorporated into the device. The markers may be included on the implanted partitioning device and/or on the delivery system. Radio-opaque markers may be constructed from biocompatible heavy metals, such as gold, platinum and tantalum, and may be fabricated in any form or shape suitable for the intended device, such as bands, tabs, ribbons, disks and the like. They may be in the form of components specifically included for the purpose of providing radio-opacity, or they may be inherent components of a device, made out of a radio-opaque material to provide radio-opacity. In some embodiments, as shown in While particular forms of the invention have been illustrated and described herein, it will be apparent that various modifications and improvements can be made to the invention. Moreover, individual features of embodiments of the invention may be shown in some drawings and not in others, but those skilled in the art will recognize that individual features of one embodiment of the invention can be combined with any or all the features of another embodiment. Accordingly, it is not intended that the invention be limited to the specific embodiments illustrated. It is intended that this invention to be defined by the scope of the appended claims as broadly as the prior art will permit. Described herein are devices, systems and methods for delivering an endocardial device. The systems for delivering the device transvascularly may generally include an elongate guide catheter having a proximal end and a distal end; a conical dilator at the distal end of the elongate guide catheter, the conical dilator being removable to enable delivery of the ventricular portioning device; a delivery catheter having a proximal and distal end; an expansion member near the distal end of the delivery catheter and configured to expand a plurality of struts of the partitioning device; and a coupling element configured to deployably secure to a hub of the partitioning device. The systems for delivering the device transapically may generally include an elongate access sheath; an elongate delivery catheter; an expansion member; and a coupling element proximal to the expansion member and configured to deployably secure to a hub of the partitioning device. 1. A delivery system for transvascular delivery of a ventricular partitioning device into a patient's ventricle and deploying the partitioning device to reduce the effective volume of the ventricle by expanding the partitioning device from a collapsed delivery configuration into an expanded deployed configuration, the system comprising:
an elongate guide catheter having a proximal end and a distal end; a conical dilator at the distal end of the elongate guide catheter, the conical dilator being removable to enable delivery of the ventricular portioning device; a delivery catheter having a proximal and distal end; an expansion member near the distal end of the delivery catheter and configured to expand a plurality of struts of the partitioning device by applying pressure to the collapsed partitioning device to open the partitioning device and secure it in the ventricle; and a coupling element configured to deployably secure to a hub of the partitioning device to retain the expansion member at least partially surrounded by the collapsed partitioning device prior to deployment. 2. The system of 3. The delivery system of 4. The delivery system of 5. The system of 6. The system of 7. The system of 8. The system of 9. The system of 10. The system of 11. The system 12. The system of 13. The system of 14. The system of 15. The delivery system of 16. A transvascular method of reducing ventricular volume to treat heart disease, the method comprising:
positioning an umbrella-shaped, expandable partitioning device having a reinforced membrane in a contracted configuration near the apex of a patients' ventricle using an elongate delivery catheter to which the partitioning device is releasably coupled; expanding an expansion member near the distal end of the delivery catheter to apply pressure to the proximal end region of the contracted partitioning device to expand the partitioning device; and releasing a coupling element distal to the expansion member on the delivery catheter to deploy the partitioning device. 17. The method of 18. The method of 19. The method of 20. The method of 21. The method of 22. The method of 23. The method of 24. The method of 25. The method of 26. The method of 27. The method of 28. The method of 29. A delivery system for transapical delivery of a ventricular partitioning device into a patient's ventricle and deploying the partitioning device to reduce the effective volume of the ventricle by expanding the partitioning device from a collapsed delivery configuration into an expanded deployed configuration, the system comprising:
an elongate access sheath having a proximal end and a distal end; an elongate delivery catheter having a proximal and distal end; an expansion member near the distal end of the delivery catheter and configured to expand a plurality of struts of the partitioning device by applying pressure to the collapsed partitioning device to open the partitioning device and secure it in the ventricle; and a coupling element proximal to the expansion member and configured to deployably secure to a hub of the partitioning device to retain the expansion member at least partially surrounded by the collapsed partitioning device prior to deployment. 30. The delivery system of 31. The delivery system of 32. The delivery system of 33. The delivery system of 34. The delivery system of 35. The delivery system of 36. The delivery system of 37. The delivery system of 38. A transapical method of reducing ventricular volume to treat heart disease, the method comprising:
positioning an umbrella-shaped, expandable partitioning device having a reinforced membrane in a contracted configuration near the apex of a patient's ventricle using an elongate access sheath to which the partitioning device is releasably coupled; expanding an expansion member to apply pressure to the proximal end region of the contracted partitioning device to expand the partitioning device; and releasing a coupling element proximal to the expansion member to deploy the partitioning device. 39. The method of 40. The method of 41. The method of 42. The method of 43. The method of 44. The method of 45. The method of CROSS-REFERENCE TO RELATED APPLICATIONS
INCORPORATION BY REFERENCE
TECHNICAL FIELD
BACKGROUND
SUMMARY
BRIEF DESCRIPTION OF THE DRAWINGS
DETAILED DESCRIPTION