REHABILITATION MECHANISM FOR PATIENTS CONFINED TO BED AND BED COMPRISING THE REHABILITATION MECHANISM
The present invention relates to a rehabilitation mechanism for bedridden patients and a bed comprising the rehabilitation mechanism, particularly a hospital bed, clinical bed, gurney, or intensive-care bed. Persons suffering from an illness or as a result of an accident, for example, or who are “bound” to a bed as a patient for other reasons for longer than the normal nighttime rest period (referred to below as bedridden patients) often have restrictions on activity that lead to such persons being poorly able or even unable to participate in social life after leaving the bed, that is, unable or only partially able to work and requiring assistance in daily life. Through rehabilitation, the patient can regain part of his activity. In the medical field, rehabilitation means the application and effects of measures intended for reducing to a minimum the physical, psychological, and social consequences of a handicap or limitation on activity (formerly: disability, now: activity) and interruption of participation (formerly, handicap; now, participation) in social life. Medical rehabilitation has been proven to be particularly significant for the human locomotor system. If the bones, joints, muscles, and tendons, particularly of the human legs (comprising the buttocks, hip joint, thigh, knee joint, calf, and foot) are not moved regularly, they will stiffen—the related locomotion centers located in the human spinal tissue can atrophy. Unlike persons who are physically able and have a stable circulatory situation allowing participation in treadmill training, for example, said training is typically denied to bedridden patients. The particular reasons can be orthopedic, intensive-care, and/or neurological limitations on activities encountered individually or cumulatively. Orthopedics is the field of activity of a specialist for orthopedics and trauma surgery and addresses the occurrence, prevention, detection, and treatment of congenital or acquired defects in the form or function of the musculoskeletal system, that is, the bones, joints, muscles, and tendons, and the rehabilitation of such patients. Orthopedic treatments include surgical methods such as particularly prosthetic surgery (e.g., but not limited to, hip or knee joint replacement). After an accident or surgical intervention, bedridden patients are typically not able to apply full body weight to the bones, joints, muscles, and tendons of one or both legs due to orthopedic limitations on activity. In order to nevertheless prevent stiffening of the legs, an in-bed exercise machine is know from WO 00/45897 A1, for example, allowing performing of cyclical leg motions in a reclined position when pushed up to the end of a hospital or clinical bed. The known in-bed exercise machine, however, particularly does not allow exercise in a vertical position. In order for the feet to be fully or partially loaded by the body's own weight, however, which can accelerate the healing process after a joint replacement or bone fracture, for example, it is necessary to be able to bring the bedridden patient completely or partially into a vertical position. Said consideration is addressed, for example, by the standing table disclosed by WO 00/61059 A1. It is thereby problematic that said standing table or comparable known devices are typically located in a separate training room, but in any case require relocating the patient from the bed to the corresponding rehabilitation device. At least for intensive-care patients, but also for patients requiring intensive-care treatment, this is generally not possible, but in any case is associated with particular risks. Intensive care is a medical specialty addressing the diagnosis and therapy of life-threatening conditions and illnesses. Intensive-care services are typically provided in specially equipped units of a hospital or clinic, known as intensive-care units, led by specially trained specialists such as anesthesiologists, internists, surgeons, or neurologists. The results of intensive-care services cover a wide range, depending on the underlying illness. In principal, there must be a certain positive prognosis of the illness condition. The goal of intensive-care services is namely to restore full health or at least to achieve a largely autonomous condition for the patient. So-called life-extending measures, therefore, are not pursued for their own sake. Patients are admitted to intensive-care units whose condition is life-threatening or could become life-threatening, particularly due to a weak cardio-circulatory system, risk of cardiac arrest, infection risk, and the like. Said fact is addressed in standardized monitoring measures in intensive-care units. Intensive-care units have extensive technical building structures and equipment. A focal point is the design of the intensive-care bed, which serves for safely supporting the most ill patients in intensive-care units. In addition to apparatus supporting the monitoring measures, an intensive-care bed is particularly characterized by a mattress suitably designed for preventing bedsores and for immediately manually resuscitating at least the heart and/or lungs of an intensive-care patient. The mattress must also be non-conductive for performing defibrillation and resistant to liquids, blood, and wipe-down disinfection using commercially available disinfecting agents. In order to secure intensive-care patients against falling out of bed, the mattress is usually enclosed by barriers on the long and transverse sides that can be attached to the long and transverse sides of a bed or mattress frame and often support at least part of the monitoring apparatus. Due to said typical design of intensive-care beds, the known rehabilitation devices described above cannot be easily brought adjacent to a modern intensive-care bed and/or require repositioning of the patient. The latter, however—as has already been mentioned—is typically not possible for intensive-care patients, who are normally weak or require intensive-care services for other reasons, but in any case is associated with special risks. Meanwhile, patients in intensive-care units already have a five to ten times higher risk of infection in comparison with patients in normal units. Various infection-promoting factors add up for intensive-care patients, originating both from the patients themselves and from the treatment measures using in intensive care (many catheters, tubes, etc.) Therefore, in order to reduce the risk of infection, special hygienic measures are specified for intensive-care unit, and rehabilitation devices such as the known in-bed exercise machine or known standing table meet such specifications only with difficulty. Rehabilitation strategies supported by rehabilitation devices therefore have typically been first used up to now after the patient has left the intensive-care unit. Neurology is the study of diseases of the nervous system. The organ system that are addressed in neurology are the central nervous system, that is, the brain and spinal cord, surrounding structures and blood-supply vessels thereof, and the peripheral nervous system including structures thereof connecting to the muscles, and the musculature. For neurological rehabilitation, recent studies have shown that rehabilitation should begin as early as possible. In order to maximum the success of rehabilitation, for example, rehabilitation measures should be started 24 hours after a stroke exhibiting unilateral or other paralysis, or a traumatic brain injury with or without quantitative loss of consciousness, presenting as a coma in the most severe form. Because patients affected by paralysis and/or loss of consciousness are typically still in an intensive-care unit at this point in time, the neurological rehabilitation strategies to be begun at an early point are doubly difficult: in addition to the intensive environment describe above, which is problematic in itself, the entire leg motion must be performed cyclically solely by the rehabilitation device, at least for paralyzed and/or comatose patients, at least at first. For these reasons, exercises for maintaining activity of patients in intensive-care facilities are mostly performed by special physical therapists who manually move the limbs of intensive-care patients—daily if possible, but at least several times a week. Said manual physical therapy is disadvantageous in that the therapists can fatigue quickly due to the physical exertion, leading to difficulty in planning, let alone evaluating, session progress. Furthermore, it is not guaranteed that the physical therapist will work at the same (maximum) effort and efficiency for every physical therapy session. The physical therapist also cannot perform an objective quantification of the activity of the patient, only subjective, making objective quantification of the success of the therapy over several therapy sessions difficult. Finally, a therapy session, particularly in the intensive-care environment, can require not only the presence of one or more physical therapists, but also the presence of a nurse who must monitor the vital parameters of the patient [90] during the session, for example in order to be able to react to cardiac circulatory problems. The additional presence of highly qualified clinical personnel causes such therapy sessions to be unaffordable. On this basis, the object of the present invention is to provide an improved rehabilitation mechanism in comparison with the prior art, particularly for patients having become bedridden due to orthopedic, intensive-care, and/or neurological limitations on activity, allowing planned, automated rehabilitation of at least the joints, muscles, and tendons of the legs of bedridden patients without requiring bed-to-bed transfer of the patient. In addition to commercially available or self-built hospital or clinical beds, the rehabilitation mechanism should also be usable in commercially available or self-built gurneys or intensive-care beds, regardless of whether the bedridden patient can be brought into a partially or completely vertical position in the corresponding bed, wherein the rehabilitation mechanism can support a rhythmic loading and unloading of the soles of the feet of bedridden patients in any position of the bedridden patient between a horizontal and a vertical position. Said object is achieved first by a rehabilitation mechanism having the features of the independent claim 1. A rehabilitation mechanism according to the invention implemented for planned, automated rehabilitation of at least the joints, muscles, and tendons of the legs of a bedridden patient, comprises at least:
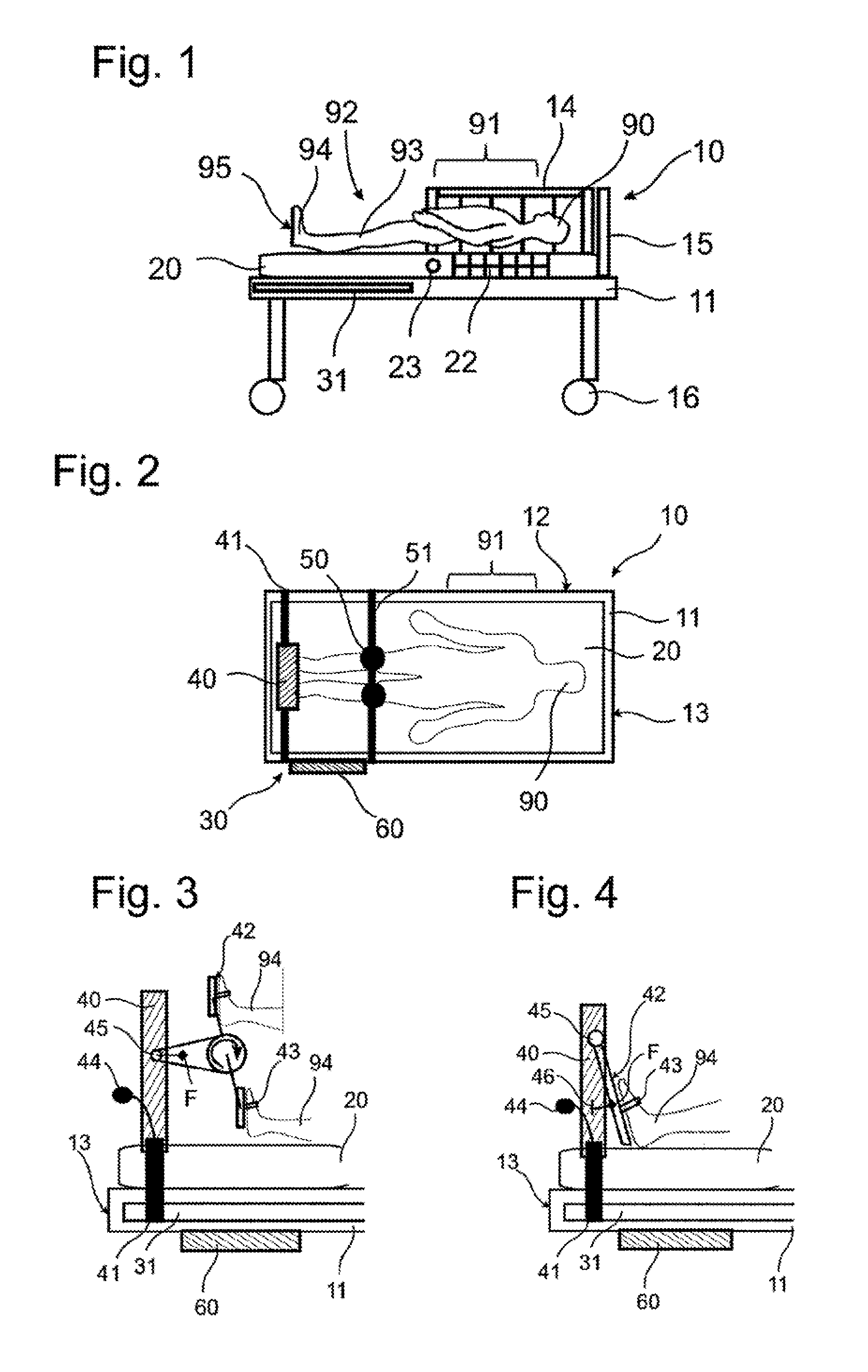
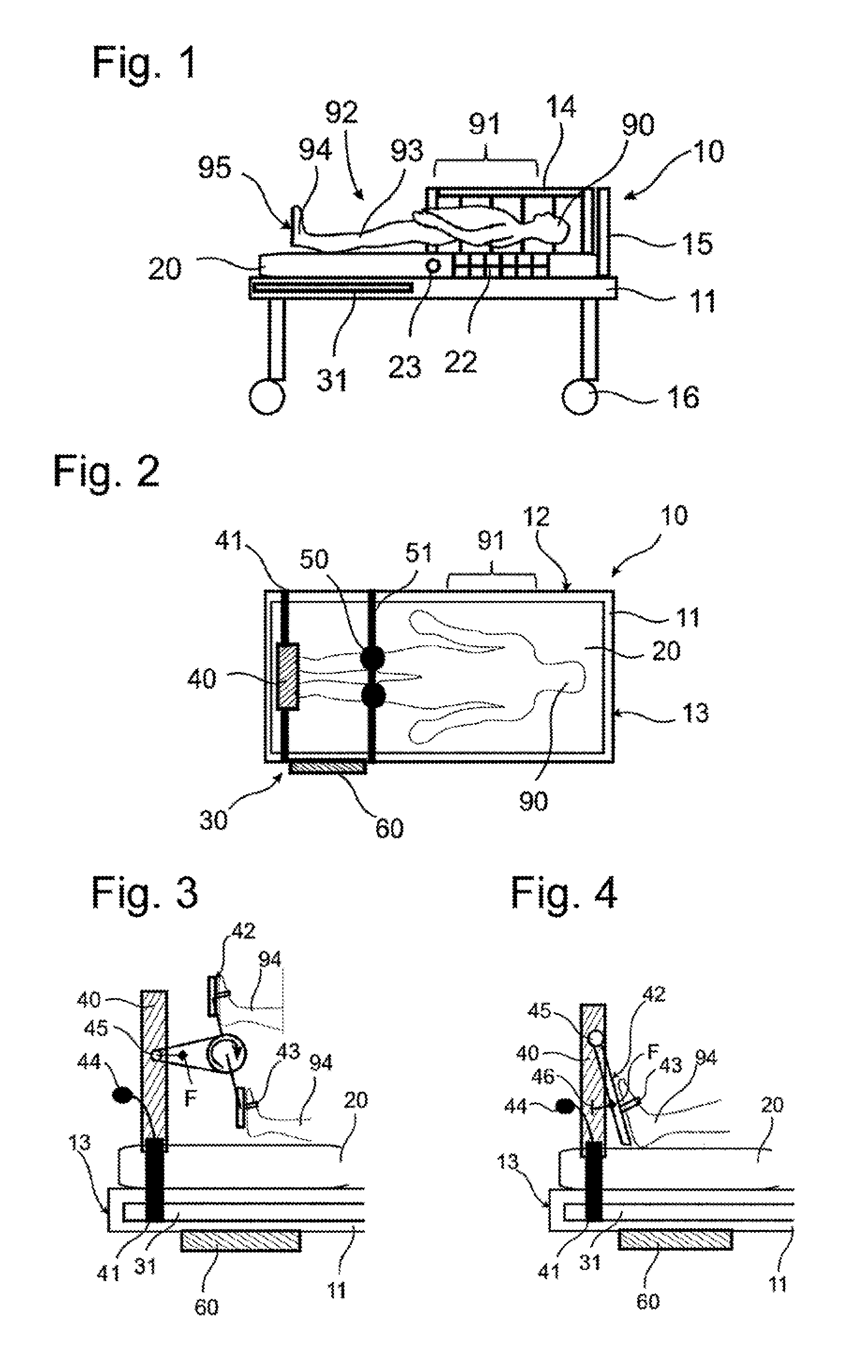
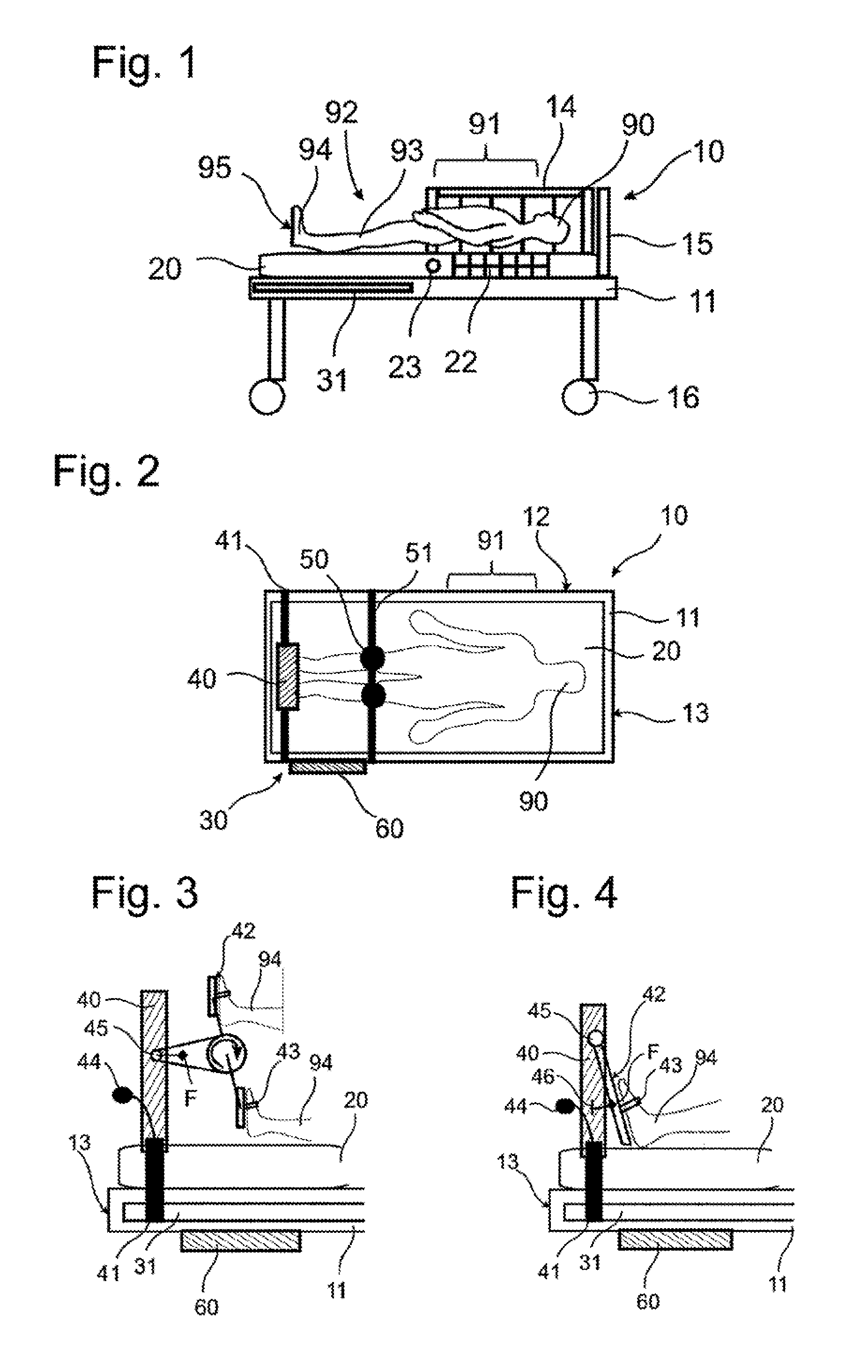
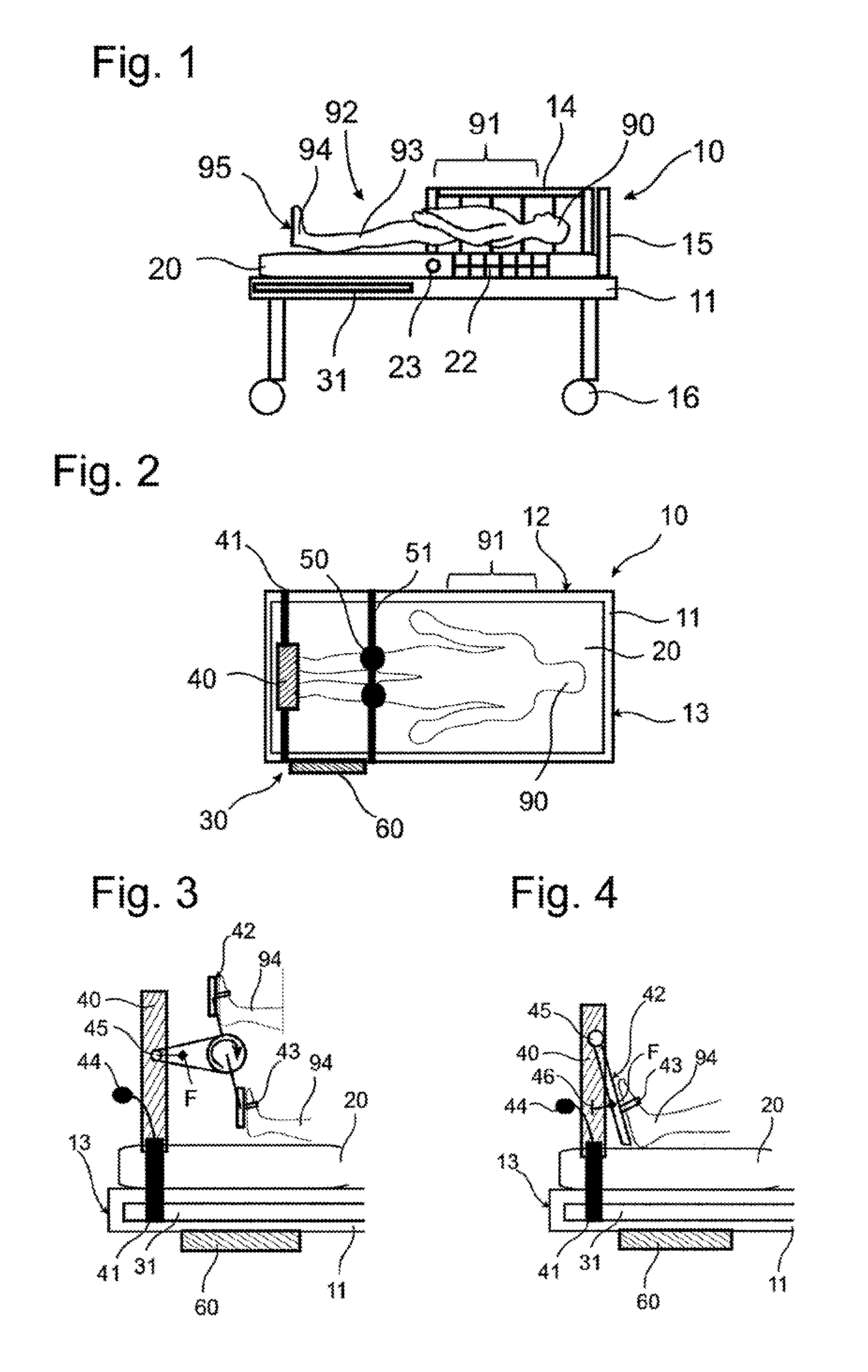
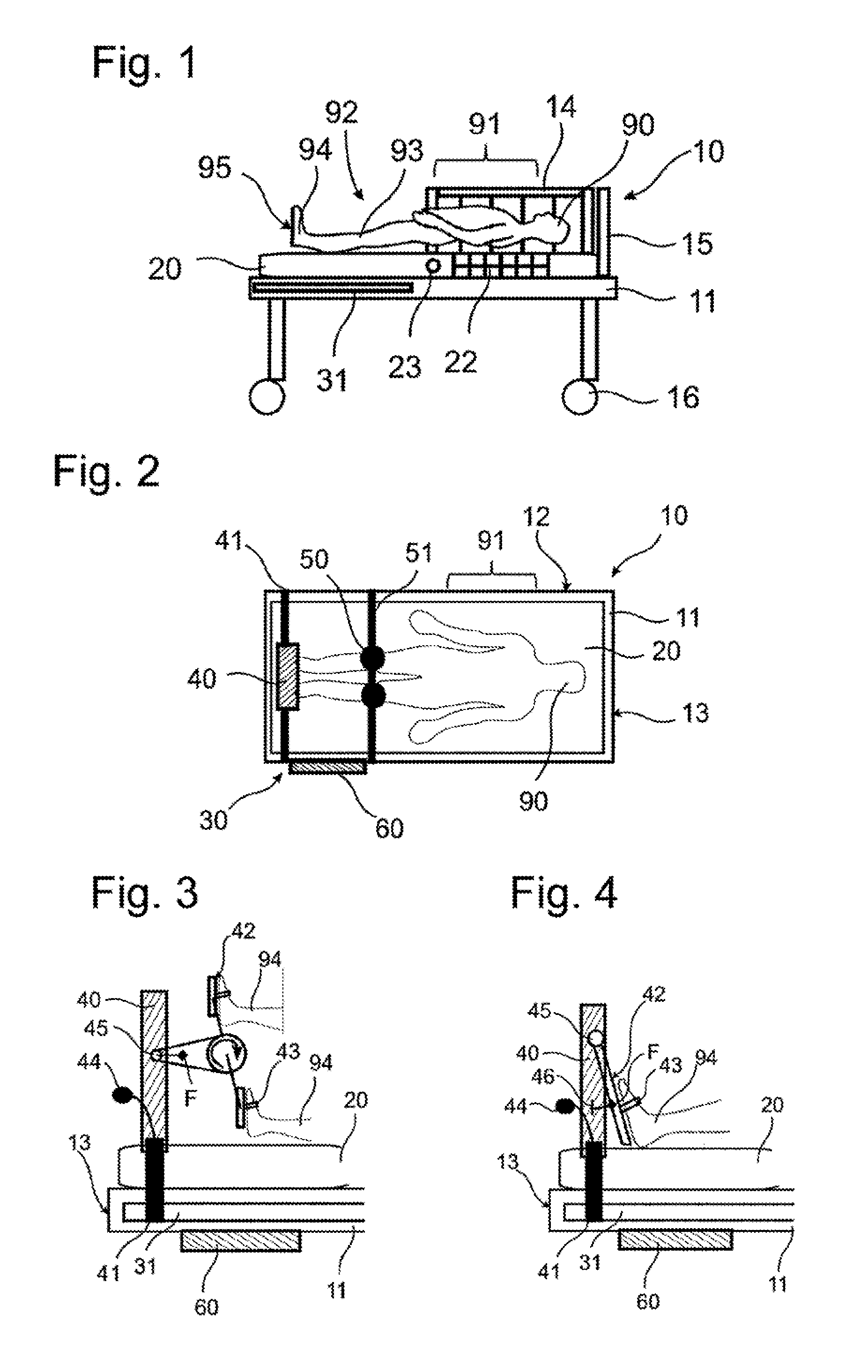
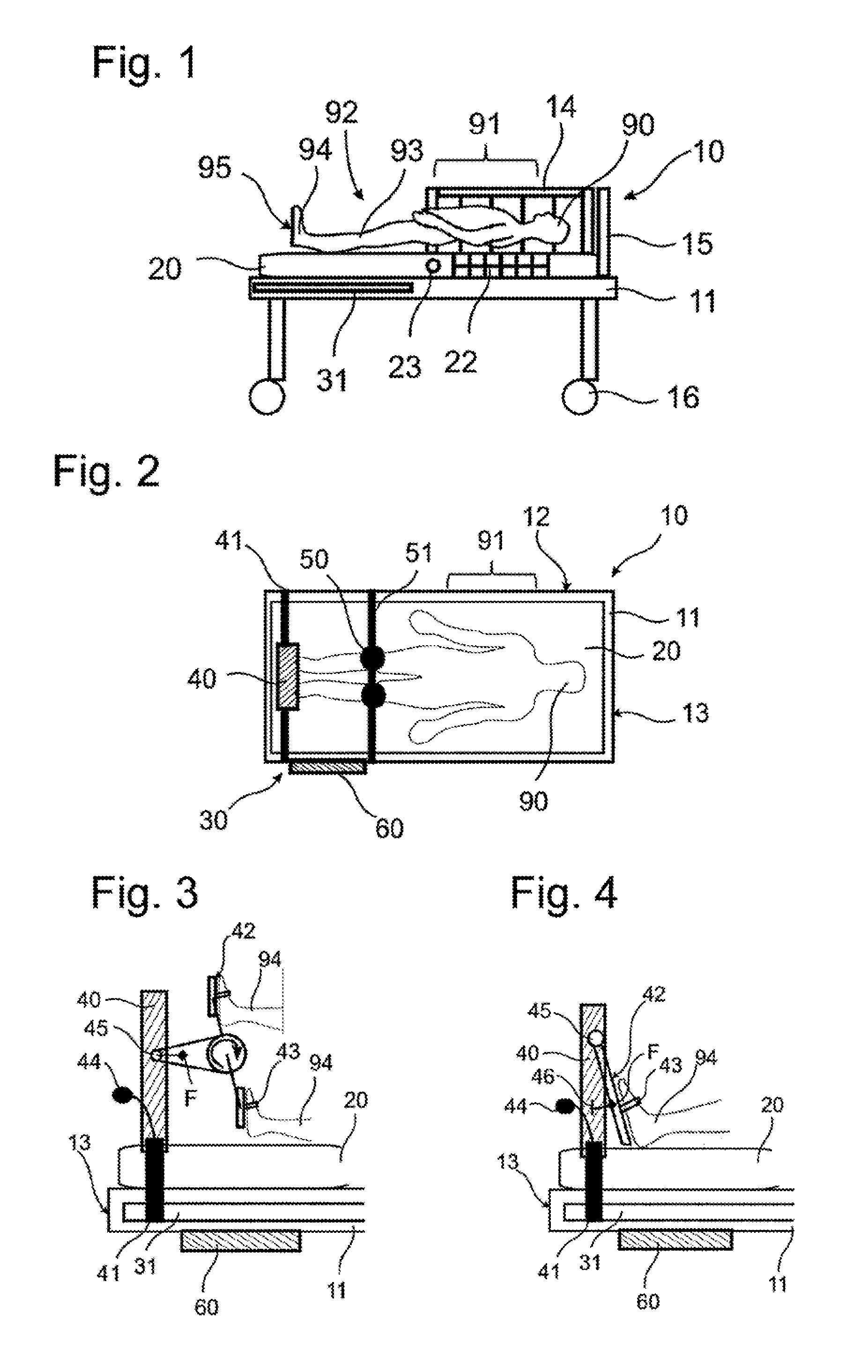
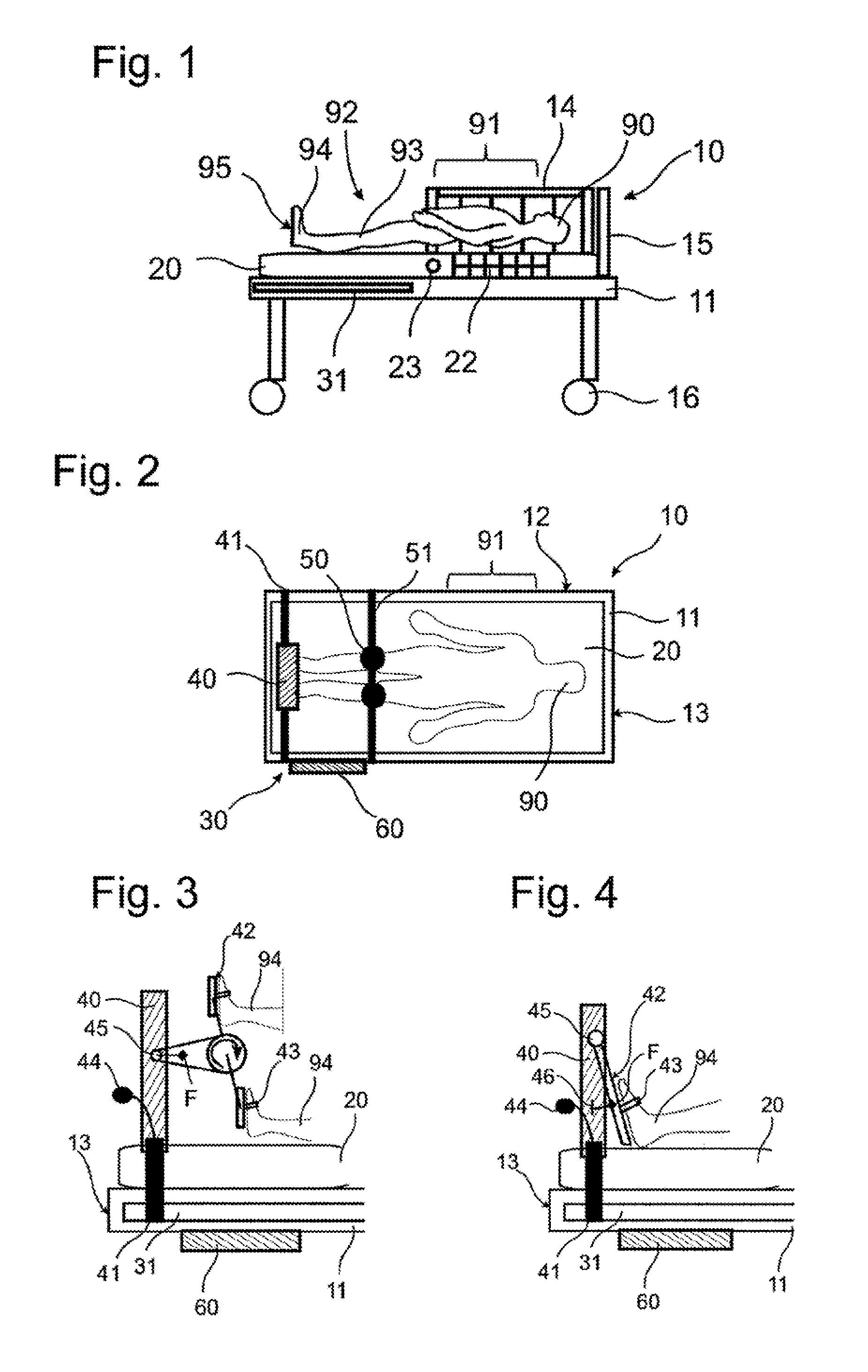
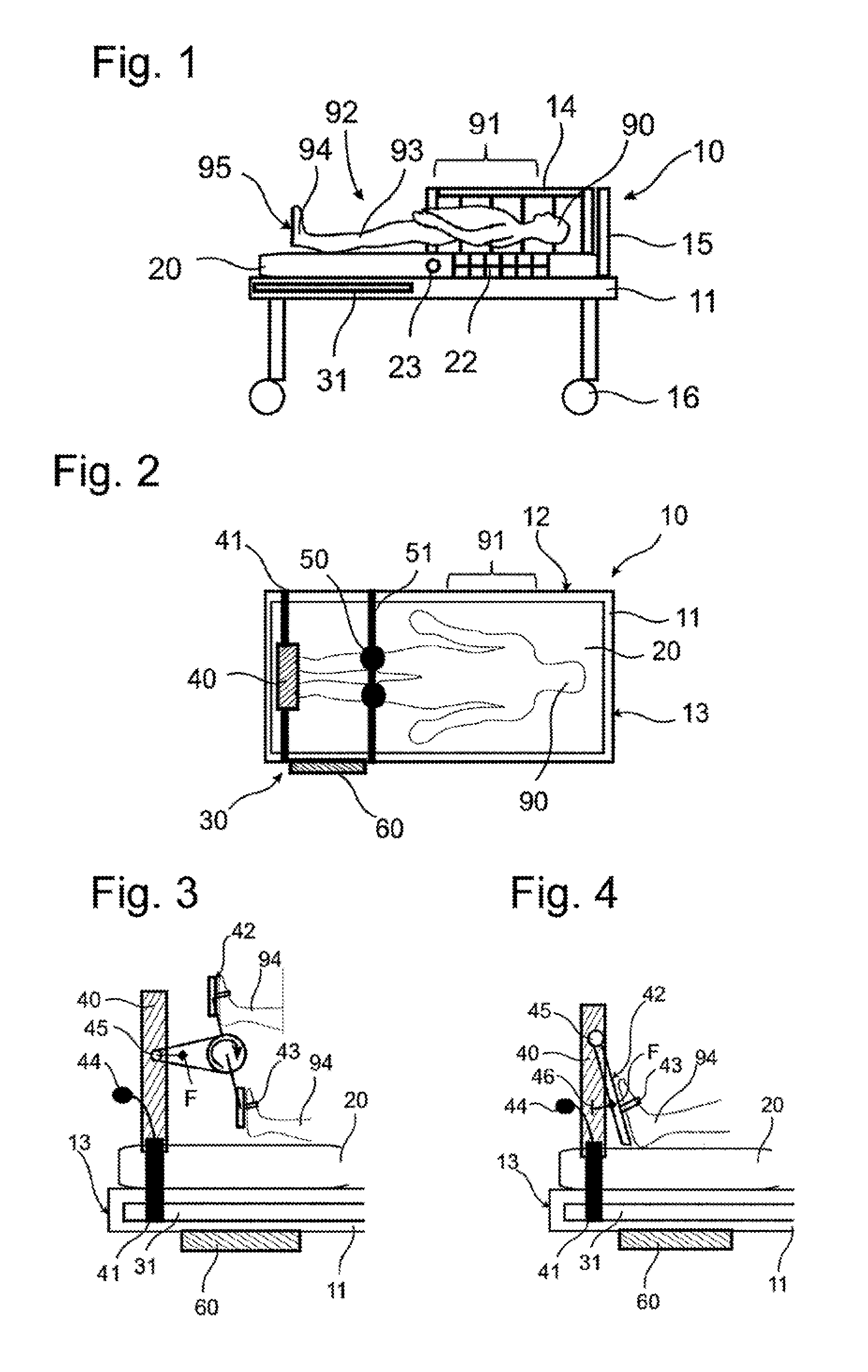
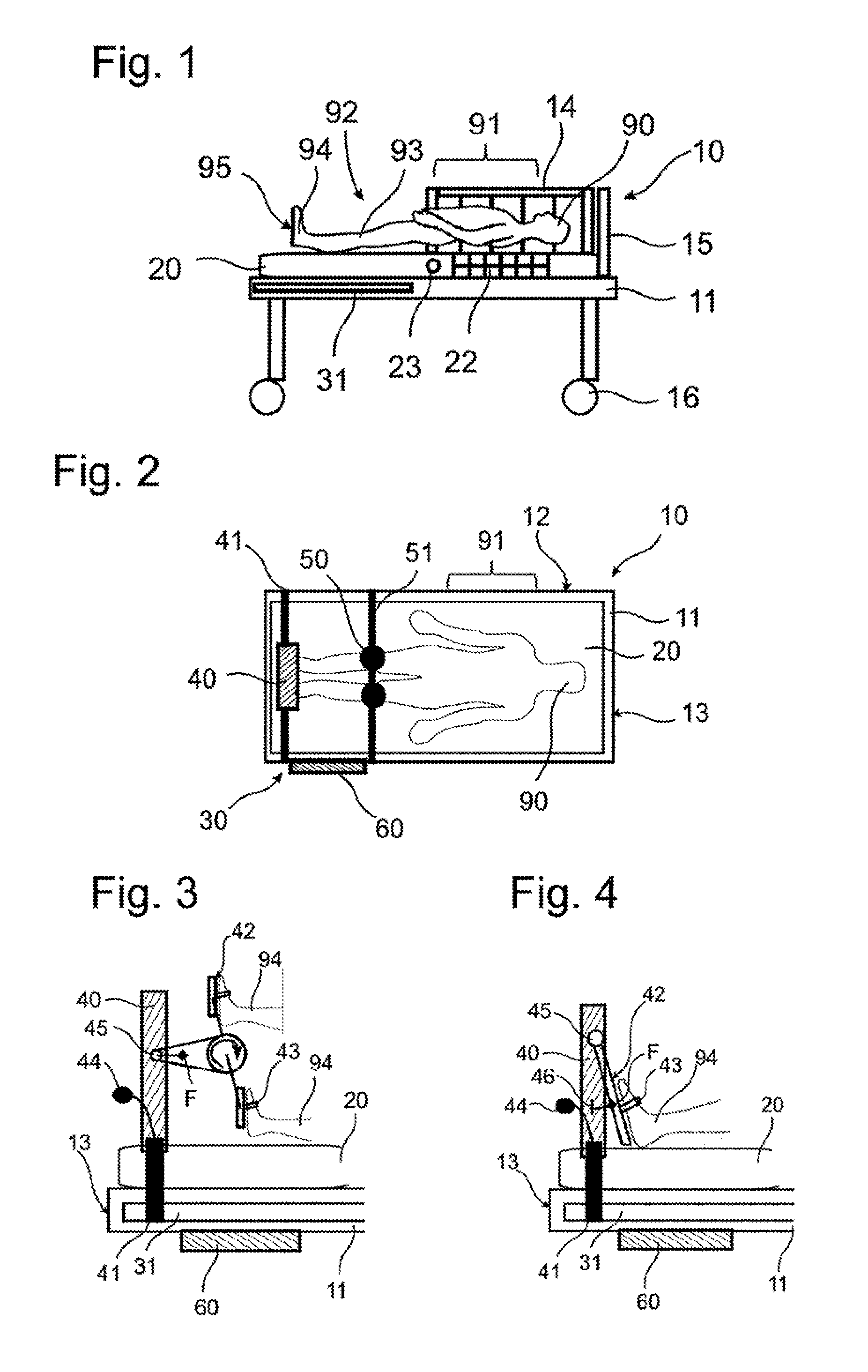
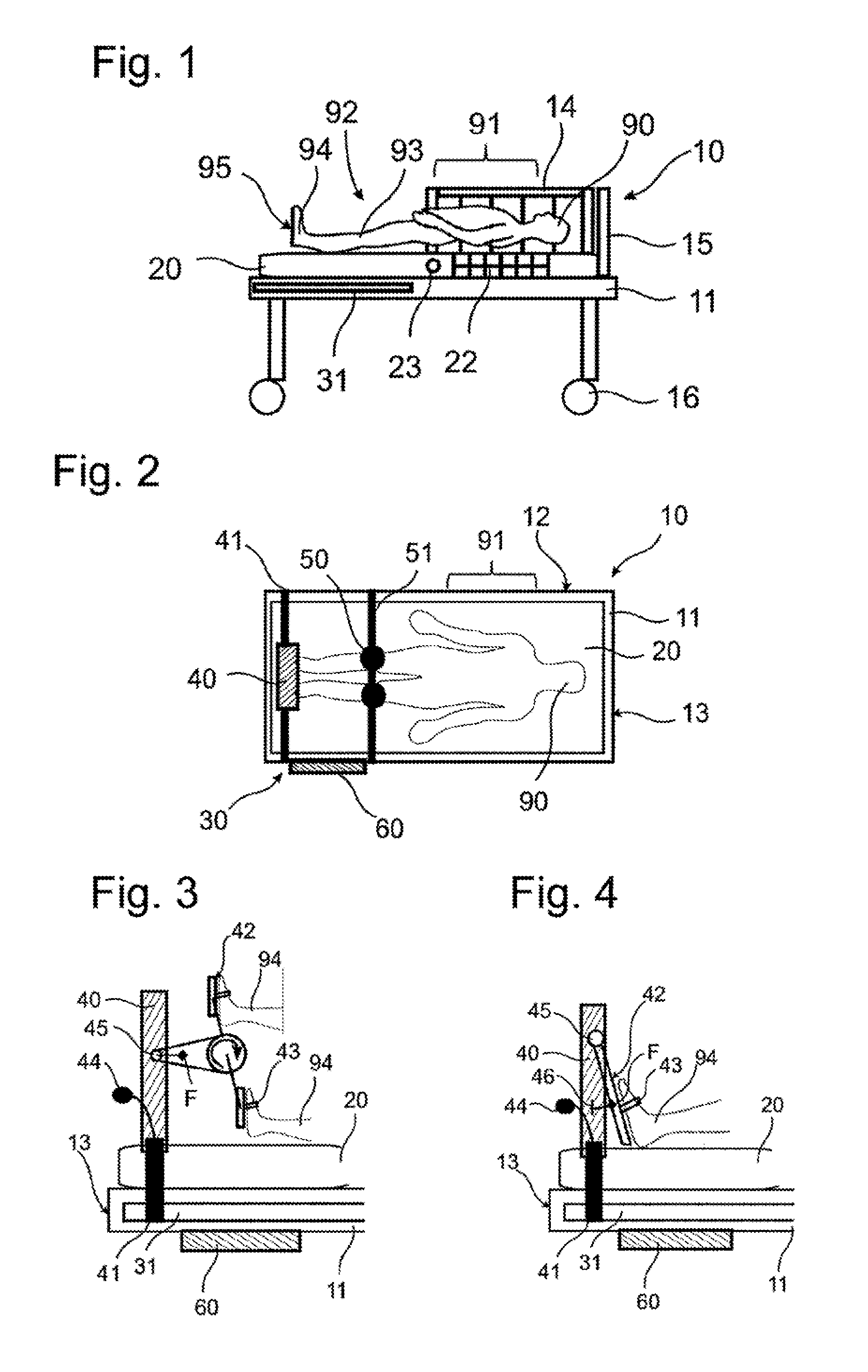
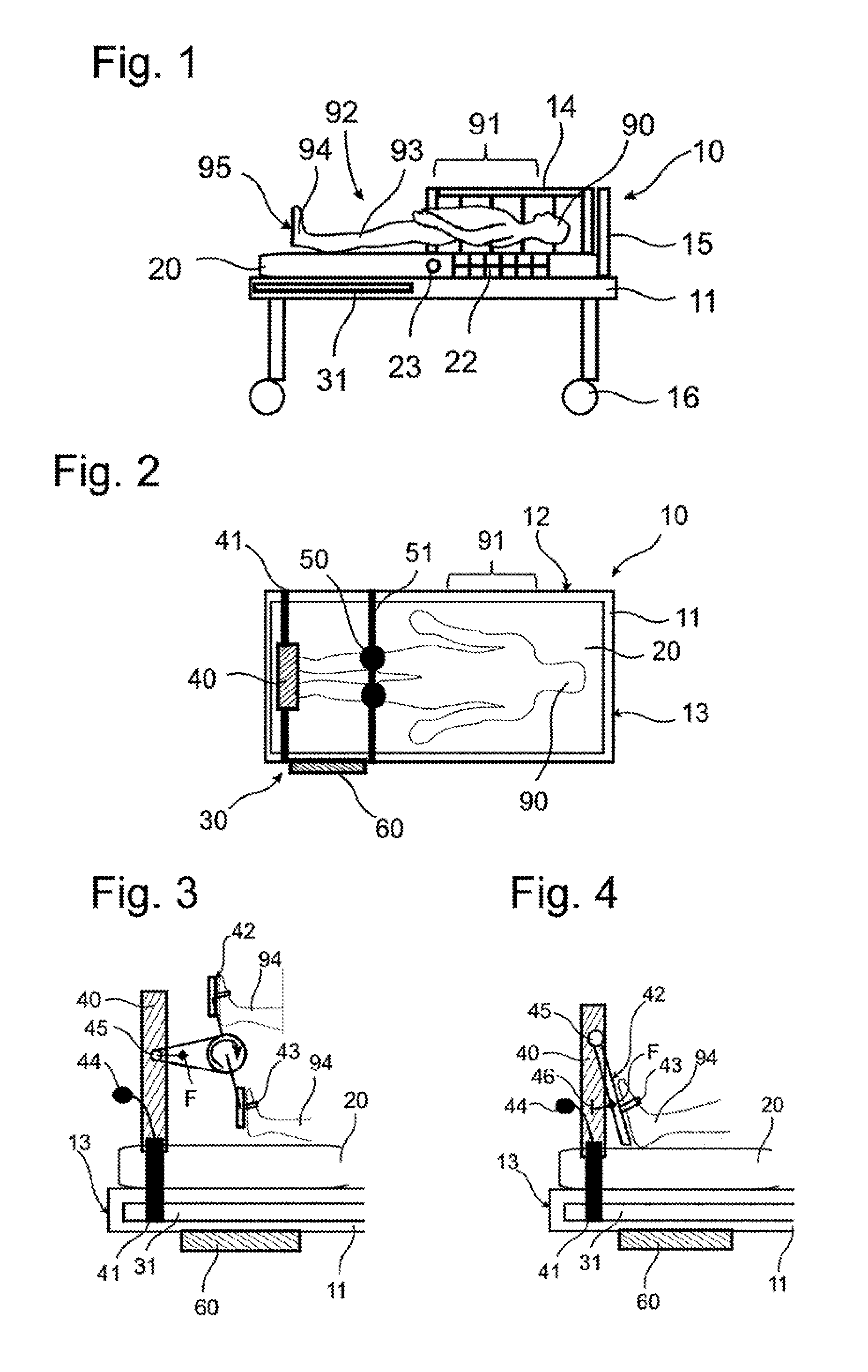
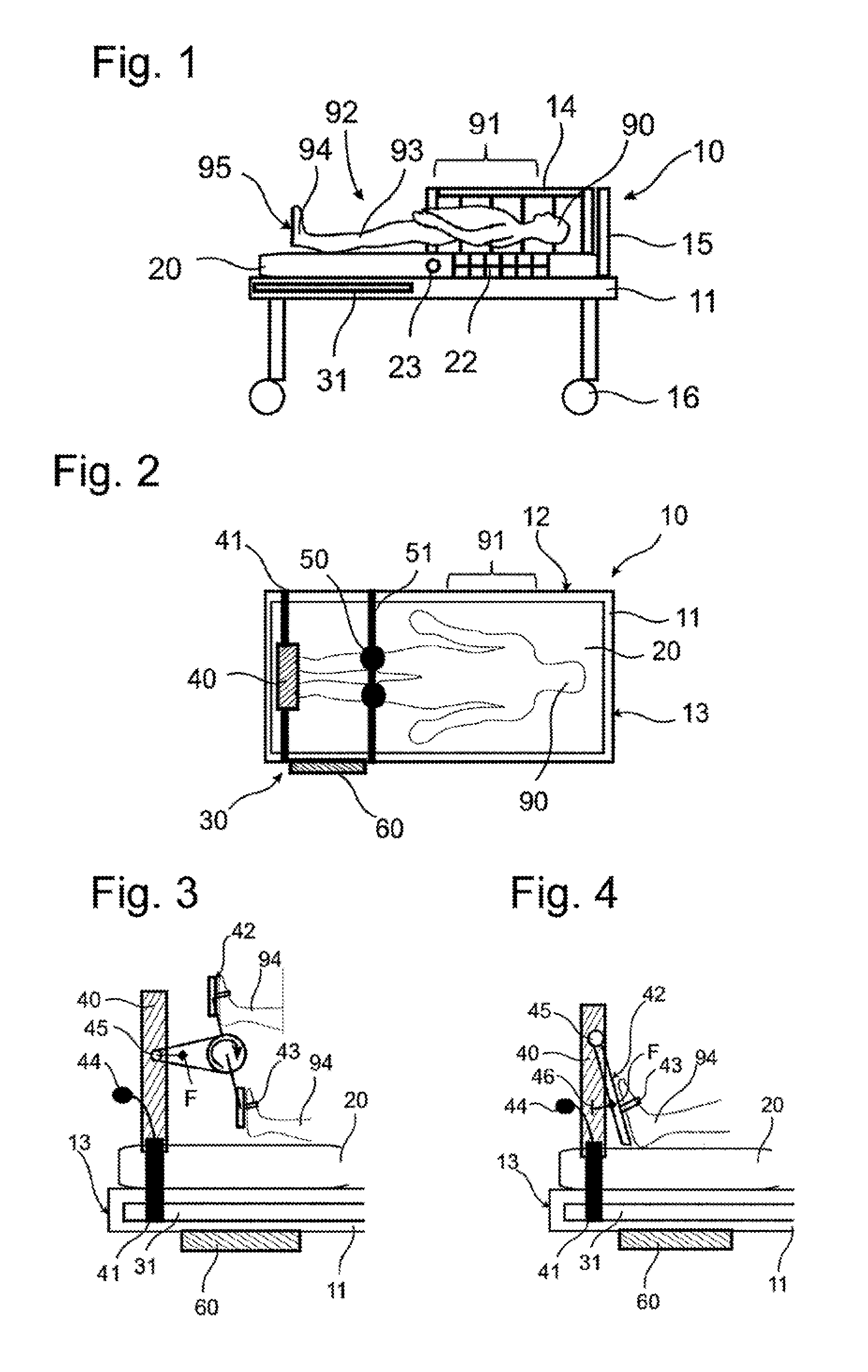
The invention is further characterized in that at least the knee module is implemented as a module for disposing between the patient and the mattress and supported directly or indirectly on a bed or mattress frame. The modular design of the rehabilitation mechanism has the advantage that bedridden and particularly intensive-care patients can receive planned, automated rehabilitation directly in the bed, without requiring high-risk transfer between beds and/or the ability to cooperatively contribute. The term “module” or “modular design” should be understood hereafter particularly such that components so designated form individual, self-contained assemblies, indeed operatively connected to further elements but reversibly separable for the purpose of storing and/or transporting. The modules, particularly the foot module and the knee module, are fully mechanical and electrically separable form a bed on which said modules are used and can thus be stored separably. Alternatively or additionally, said modules can be folded away, for example in a space beneath a mattress of a bed. The modularity, removability, or separability of the foot and knee module from the bed, whether by separating or by storing the therapy module beneath the bed, is particularly advantageous because the bed can be used as a normal bed outside of the therapy periods. The term “normal use” is understood thereby to mean that no element of the rehabilitation mechanism prevents access to the patient from all sides in any form, prevents the transfer from or into the bed, or prevents or hinders any necessary emergency measures or care measures. The rehabilitation mechanism can preferably be reversibly releasably fixed to a hospital bed, in particular a conventional hospital bed. Said mechanism is provided and set up for reversibly disposing on conventional hospital beds in order to thus provide therapy for a patient lying in the bed. The rehabilitation mechanism preferably comprises support and/or clamping means in order to achieve reversible fixability. The rehabilitation mechanism can preferably be removed from a hospital bed as a module, particularly from a conventional hospital bed, and/or can be stowed beneath the hospital bed. The use of the rehabilitation mechanism is thereby substantially simplified. Said module is a self-contained system usable selectively on existing hospital beds. Disposing a knee module between the patient and mattress and supporting the same directly or indirectly on a bed or mattress frame particularly makes it possible to apply supporting force to the knee joints of bedridden patients, advantageously rhythmically loading and unloading the soles of the feet of said patients, in any position assumed by the patient between a horizontal and a vertical position. For orthopedic patients, the rhythmic loading and unloading of the soles of the feet is important, for example to accustom an injured joint to walking again and/or to a load in a partially or fully vertical assumed position. For intensive-care patients, the rhythmic loading and unloading of the soles of the feet is significant in order to prevent stiffening of the legs and atrophy of the locomotion centers located in the spinal cord. For neurological patients, the alternating motion generates additional sensory input in the soles of the feet, said input being transmitted to the central nervous system. Said “efferent sensory input” ensures that the brain regions involved in generating walking motions are also excited. The planned automated rehabilitation of at least the joints, muscles, and tendons of the legs of bedridden and particularly intensive-care patients by means of a rehabilitation mechanism according to the invention has the objective of limiting to a minimum the limitations on activity and/or interruption in participation in social life. The underlying central therapeutic idea is to quantify and/or control to a desired level the activity of bedridden or particularly intensive-care patients as early as possible, that is, while still in bed. The determining of individual parameters of a planned automated rehabilitation in this respect in the course of the present invention is nevertheless the responsibility of physical therapists or at least comparably trained technicians in practice. The rehabilitation is particularly preferably a walking motion, a stepping motion, and/or a motion simulating stair-climbing. A walking motion, stepping motion, or motion simulating stair-climbing is substantially more advantageous for rehabilitation than a bicycle-riding motion, for example. A pure foot module allowing a bicycle-riding motion is known from DE 41 13 135 A1, for example. It is much more important, however, for rehabilitation patients to acquire a walking motion, stepping motion, or motion simulating stair-climbing and to simulate the loads occurring during such a walking motion, stepping motion, or motion simulating stair-climbing, and to measure progress thereby. A bicycle-riding motion is suitable only under certain conditions, as here in particular no rolling of the foot occurs and a torque applied to the ankle joint of the foot tends to be low. According to the invention, the foot module and the knee module together form an exoskeleton for the patient. The modules forming the exoskeleton act together by means of the control module and support the patient in performing the motion. The rehabilitation mechanism further preferably comprises a biofeedback module for providing a visual and/or audible feedback to the patient. Such a biofeedback module preferably comprises a display or the like disposed in the field of vision of the patient in order to give said feedback. Such a biofeedback module can fundamentally be implemented as disclosed in US 2010/0042022 A1. Said module is preferably implemented for indicating to the patient whether said patient is performing a motion properly and/or is making progress. The biofeedback module is further preferably implemented for indicating to the patient that said patient is not performing a motion correctly, should change exercises, should stop an exercise, and the like. The object of the present invention is therefore also a bed comprising the rehabilitation mechanism according to the invention, wherein said bed can be implemented as a commercially available or self-built hospital bed, a clinical bed, a gurney, or particularly an intensive-care bed. Advantageous embodiments and refinements, usable individually or in combination with each other, are the objects of the dependent claims. Said details and additional details and further advantages of the invention are described below using preferred embodiment examples, to which, however, the present invention is not limited, and in conjunction with the attached drawing. They show schematically: In the description below of preferred embodiments of the present invention, identical reference numerals indicate identical or comparable components It is evident how in a first preferred embodiment of the rehabilitation mechanism 30 said module comprises a foot 40 and a knee module 50 implemented as modules for disposing above the mattress 20 and for directly or indirectly supporting on a bed 11 or mattress frame 21. An advantage thereof is that commercially available, particularly non-divided and easily cleaned and disinfected mattresses 20 can be used, because (unlike particularly the standing table mentioned above), as said mattresses need not make space for mechanics. In addition, when rehabilitation is not taking place, the foot 40 and knee module 50 can be advantageously removed from the bed 11 or mattress frame 21, whereupon the bed 10 functions as a standard bed 10, such as a hospital bed, clinical bed, gurney, or intensive-care bed. The removed modules can be stowed on or under the bed 10, for example, until the rehabilitation is continued—optionally after prior cleaning or disinfection—or preferably used in the meantime for performing further planned automatic rehabilitations on other bedridden patients 90, whereby the investment costs incurred for the rehabilitation mechanism 30 are advantageously amortized more quickly. In order to be able to operatively connect the foot module to the feet 94 and to operatively connect the knee module 50 to the knee joints 93 of the bedridden patient 90, in a further preferred embodiment of the rehabilitation mechanism 30 according to the invention the foot 40 and the knee module 50 are implemented as modules for fixing on both of the long sides 12 of the bed 10. The ability of the foot 40 and/or knee module 50 to be fixed can be provided in a low-cost embodiment by means of two guide rails 31, each of which can be mounted on one long side 12 of the bed 11 or mattress frame 21 and thus advantageously allow retrofitting for a plurality of existing beds 10. For fixing variably along the long sides 12, the foot 40 and the knee module 50 can comprise suitable fixing means 41 and 51 by means of which the modules 40 and 50 can advantageously be operatively connected to the feet 94 and knee joints 93 of the bedridden patient 90 corresponding to the anatomical conditions. In order to handle different widths of beds 10 and/or special anatomical considerations of the bedridden patient 90, fixing means 41 and 51 variably adjustable in not only the longitudinal direction but also the transverse direction of the bed 10 are finally preferred. In a further preferred embodiment of the rehabilitation mechanism 30, the foot 40 and/or the knee module 50 can be electromechanical in design. A complete or partial electromechanical design of the foot 40 and/or knee module 50 has the advantage that electric motors can be actuated very simply and very precisely. Electric motors 45 or other actuators 53 (in contrast to pneumatic compressors, for example) are also relatively low-noise. Electromechanical drives can also be displaced very quickly, which can be advantageous in an emergency situation. Alternatively or cumulatively thereto, in a further embodiment of the rehabilitation mechanism 30 the foot 40 and/or the knee module 50 can have a fluid-dynamic design. A complete or partial fluid-dynamic design of the foot 40 and/or knee module 50 has the advantage that the force transmission to the patient 90 can be generated by means of cushions 57, for example, being expanded and/or contracted via a hose system 58 by means of a vacuum pump 59. Said design would distribute the compressive and tensile forces F required for the motion of the legs 92 over a larger area on the patient 90, thus preventing risks of injury as the force F cannot be transferred at points potentially having greater intensity, but rather over a larger area having a lower point force. The above is shown more clearly using the embodiment examples shown in the following It is evident how the foot module 40 can be constructed similarly to a fitness stepper, for example. To this end, the bedridden patient 90 typically puts on shoes. The step surfaces 42 of the foot module 40 can also be designed, however, so that training can be performed barefoot or in socks. The feet 94 can be fixed to the foot module 40 by means of elastic fixing bands 43, similar to a snowboard binding or the like. It is thus ensured that the soles of the feet 95 of the bedridden patient 90 make contact with the step surfaces 42 of the foot module 40 independently of any vertical position. In a further embodiment, the foot module 40 can comprise an adjusting lever 44 by means of which the distance between the step surface 42 and the sole of the foot 95, for example, can be finely adjusted. The foot module 40 can have a mechanical and/or electromechanical design. In the mechanical variant, a bedridden patient can—assuming appropriate consciousness and fitness—can push against a mechanism and/or damping elements For an electromechanical variant, an electric motor 45 provides complete or partial support force, particularly at the level to which the bedridden patient is not able to independently execute motions of the legs 92 and/or load the soles of the feet 95. Finally, combined embodiments of a foot module 40 are also conceivable, wherein for example a mechanism can have supporting force from an electric motor connected or disconnected, or vice versa. According to said embodiment example ( It is important for implementing a walking motion, stepping motion, and/or motion simulating stair-climbing that the device ensures that the foot can roll during the walking motion, stepping motion, and/or motion simulating stair-climbing, that is, the foot does not set down flat on the heel and tip at the same time, but rolls from the front part of the tip of the foot, across the middle of the foot, to the heel. For one thing, the loading situation on the patients body is thereby closer to natural loading when a foot module similar to a bicycle (cf. The embodiment examples according to Unlike the foot module 40, which can also be purely mechanical and particularly passive in design, a knee module 50 according to the invention is intended to continuously advantageously apply supporting forces just below, directly at, and/or just above the knee joint 93. The knee module 50 is inserted between the mattress 20 and the patient 90 beneath the knee joints 93 thereof and fixed to the bed 11 or mattress frame 21 for executing planned rehabilitation motions. Common to the embodiment examples according to Also common to the embodiment examples according to In order to prevent overextending the knee joint 93, the cushions 57 can be controlled so that a residual amount of fluid remains in the cushion 57. To prevent excess expansion of the cushion and/or of the hose system 58, an overpressure valve set to a maximum threshold pressure can further be provided. It is ultimately critical for the controlling of planned rehabilitation motions that the foot module 40 as well as the knee module 50 can be adapted to the anatomical conditions of the bedridden patient 90 in an individual home position of the patient 90 in which the legs 92 thereof take on an extended position aligned flush to each other. To this end, a final position can be finely matched, even perpendicular to the mattress 20, for example by means of the lever 44 provided on the foot module 40. Alternatively or cumulatively thereto, the actuators 53 of a knee module 50 having an electromechanical design can be displaced to a flush point of said home position, from which the planned rehabilitation motion can be executed and controlled. For a knee module 50 having a fluid-dynamic design, the cushions 57 can be implemented having a base fill level or a base-filled chamber system, wherein the base filling in turn corresponds to the desired flush point of said home position. In a further preferred embodiment of the rehabilitation mechanism 30, said mechanism comprises at least one sensor F, EMG, by means of which a quantification of any self-contribution by bedridden patients 90 during planned automated controlling of rehabilitation motions is made possible by measuring compressive forces F at the soles of the feet 95 of the patient 90 and/or by measuring compressive and/or tensile forces F at the knee module 30 and/or by measuring muscle activity EMG in the legs 82 of the patient 90. An objective clinical qualification of the change (improvement) can thereby be performed of the ability of the patient 90 to independently generate the forces required for the motion. Considered over the time period for rehabilitation (typically a plurality of days to weeks), said quantification can then provide insight into the rehabilitation process and success thereof. Based on said data provided by the at least one sensor F, EMG, the specialists (physicians, physical therapists, or the like) can adapt, or plan, the automated rehabilitation motions, particularly with respect to the methodology and/or intensity for each patient 90 over the course of the rehabilitation process. In a further preferred embodiment of the rehabilitation mechanism 30, the control module 60 accesses compressive and/or tensile force measurement signals and/or EMG measurement signals for executing planned automated rehabilitation motions. The rehabilitation motions can thereby be performed automatically, so that the patient 90 obtains the right amount of support force at the right time. Or, in other words, the bedridden patient 90 obtains a support force only in the part of the motion cycle in which he requires support. The rehabilitation mechanism 30 behaves “transparently”, in contrast, in the part of the motion cycle in which the patient 90 can perform motions without help, that is, said mechanism merely follows the motion of the patient 90 without applying any force. Executing, that is, determining the support force required in each case, can be performed by measuring the compressive and/or tensile forces F and processing them in the control module 60 so that the rehabilitation mechanism 30 applies exactly the amount of force to the patient 90 that the patient 90 requires in order to perform the motion, but no more. Said concept can be referred to as “assist as needed.” The active participation of the patient 90 can be maximized for the first time by means of monitoring and controlling. This is primarily done by measuring the activity of the legs as a function of the load applied to the patient 90 and held to a desired level by closed-loop control Quantification of the patient's 90 own contribution can take place by measuring compressive forces on the soles of the feet 95 of the patient 90 and/or by measuring muscle activity in the legs 92 of the patient 90. Monitoring and controlling patient activity is advantageous in that the patient 90 can be rehabilitated to the limit of his load-bearing capacity. Planned automated motions at the limit of load-bearing represent substantial therapeutic progress, particularly for intensive-care and/or comatose patients 90. Said measurements also provide insight into the clinical progress of the patient 90. For safety reasons, the control module 60 continuously monitors all sensor values to that said module shuts down the rehabilitation mechanism 30 and/or emits suitable warning signals if inconsistencies or deviations from the planned rehabilitation are detected. In addition, particularly when used with coma patients 90, both the sensor side and the control side can be redundantly designed. The rehabilitation mechanism 30 according to the invention is particularly suitable for commercially available or self-built beds 10 of all kinds, particularly for hospital beds, clinical beds, gurneys, and/or intensive-care beds. In order to rehabilitate a bedridden patient 90 as close to the limit of his own ability as possible, the patients feet 94 should always bear as much of the patient's body weight as possible and thus contribute to a walking motion, stepping motion, and/or motion simulating stair-climbing. In order for the feet 94 to be loaded by the patient's body weight, it is necessary to bring the bedridden patient 90 into a vertical position. In order to ensure that the soles of the feet 95 of the bedridden patient 90 are in contact with the step surfaces 24 of the foot module 40 before vertical positioning, it is preferable to operatively connect the feet 94 of the patient 90 to the foot module prior to beginning the vertical positioning. The same applies to operatively connecting the knee joints 93 to the knee module 50. The level of vertical positioning (between 0 degrees=lying down and 90 degrees=standing) should be able to be freely adjusted as a parameter of the planned automated rehabilitation by the responsible physical therapist, that is, not only at 90° but also particularly at 45° or 60° or 75° or other arbitrary intermediate levels. A bed 10 according to the invention therefore comprises a suitably designed adjusting mechanism 70 for adjusting the mattress frame 21 at least between a horizontal and a vertical position, by means of which all other required positions than a horizontal and a vertical position can preferably also be assumed, and from which positions the mattress frame 21 can be returned to a horizontal position at any time. The adjusting mechanism 70 can comprise electric motor and/or hydraulic means for adjusting the mattress frame 21 connected to the bed frame by means of a joint, said means raising the mattress frame 21 including the mattress 20 and the patient 90 affixed thereto to the planned level of vertical positioning, for example by means of a driven angle-control mechanism. The vertical position thus assumed also advantageously allows the patient 90 to train the heart and circulatory system and to load the same optimally by adjusting the vertical positioning level according to the individual progress in healing. In order to prevent the patient 90 from falling out of the bed 10, particularly as the vertical positioning of a bedridden patient 90 increases, it is necessary to suitably stabilize the bedridden patient 90 with respect to the mattress 20. In a preferred embodiment of the bed 10 according to the invention, the stabilizing mechanism 80 therefore comprises a hip fixing element 81 by means of which the hips of the bedridden patient 90 can be fixed to the mattress 20. In order to also allow at least partial relieving of the body weight in a vertical position, it is necessary to support the body weight of the bedridden patient 90 not only by means of the patients legs 92 but also partially by means of the stabilizing mechanism 80 in order to obtain a planned relief of the body weight. The amount of the body weight to be borne by the legs 92 of the patient 90 should be able to be freely adjusted as a further parameter of the planned automated rehabilitation by the physical therapist, preferably between fully relieved (0 kg) and fully loaded (full body weight). In a preferred embodiment of a bed 10 according to the invention, the stabilizing mechanism 80 therefore comprises a support harness 82 for receiving the bedridden patient 90, a winch 83 connected to the support harness 82 and the mattress frame 21 at the head end, and a sensor F by means of which the force of the patient's body weight on the legs 92 of the bedridden patient 90 can be controlled. The sensor F can be operatively connected to the winch 83 as shown. Alternatively or cumulatively thereto, however, a force sensor F associated with the foot module 50 can provide the signal data required by the control module 60 for controlling the body weight to be applied to the feet 94 of the patient 90. Common to the embodiment examples according to In daily use, the mattress 20 of a bed 10 for bedridden 90 should prevent the bedridden patient 90 from developing wounds or even bedsores. The mattress 20 should be suitably soft in design in order to prevent such damage. In addition to suitable foam materials, an arrangement in the mattress 20 of chambers 22 particularly for fully or partially filling with air is preferred (as shown in In order to be able to return the mattress frame 21 of a bed 10 particularly implemented as an intensive-care bed in case of an emergency, a mechanism 71 for emergency horizontal positioning of the mattress frame 21 is provided in a preferred embodiment of such a bed 10. The mechanism 71 for emergency horizontal positioning preferably comprises at least one emergency lever 72, operable for example from the head and/or foot end of the bed 10 particularly implemented as an intensive-care bed, for example symmetrically on the left and right sides thereof, and particularly operable by a foot 94. By actuating the emergency lever 72, rapid lowering of the mattress frame 21 into the horizontal position can be initiated in a short time (for example in only about 5 seconds). If the mattress 20 comprises a mechanism 23 for emergency hardening, said mechanism can also preferably be activated by actuating the emergency lever 72 as described. In addition, it can be provided that in an emergency, the rehabilitation mechanism 30, that is, the foot 40 and knee module 50, immediately stop in positions in which the legs 92 of the patient 90 are extended. The emergency lever 72 is preferably operatively connected to the electric motor and/or hydraulic means and thus allows activation of emergency horizontal positioning even in case of power loss, preferably mechanically by further actuating the emergency lever 72, particularly by pressing the lever even further down, or by pulling. If the adjusting of the mattress frame 21 of a bed 10 particularly implemented as an intensive-care bed is performed by means of electric motors, the emergency horizontal positioning can be performed by means of the electric motors under normal conditions. In order to be able to perform an emergency horizontal positioning even in case of power loss, non-self-braking or backdrivable motors are preferred. If the adjusting of the mattress frame 21 of a bed 10 particularly implemented as an intensive-care bed was performed by means of hydraulic systems, then under normal conditions the hydraulics should also allow rapid lowering of the mattress frame 21. Hydraulic valves for discharging the pressure cylinders of the hydraulic system rapidly, but in a controlled manner, can be used for this purpose. In case of power failure, the values can be opened manually by actuating the above-mentioned emergency lever 72, for example. In order that bedridden or particularly intensive-care patients 90 are not subjected to excessive forces during rapid lowering of the mattress frame 21, the electric motor and/or a gearbox connected thereto for the adjusting mechanism 70 can be designed so that a predefined angular velocity is not exceeded. Alternatively or cumulatively thereto, a spring and damper system can also be provided for decoupling the motors from a mechanism in case of emergency and allowing rapid but controlled horizontal positioning of the mattress frame 21. In a preferred embodiment of a bed 10 particularly implemented as an intensive-care bed, the adjusting mechanism 70 therefore comprises an electronic angle meter 73 controlling the electric motor and/or hydraulic means of the adjusting mechanism 70 to a definable target angle and/or angular velocity. A responsible therapist or comparable specialist ensures, for planned automated rehabilitation:
Using the control module 60 (cf. Cumulatively thereto, further measurements can be performed or monitoring data can be incorporated. So-called physiological sensors for measuring muscle activity (EMG) can be provided on the patient 90, for example, particularly for checking the forces produced by the bedridden patient as calculated in the control module 60. In addition, physiological parameters such as heart rate or other vital parameters of the patient 90 can be measured and particularly controlled to a desired level, in that the level of vertical positioning of the mattress frame 21 is adjusted. This is often not possible, particularly for intensive-care beds. Thus, in addition to rehabilitation targets, care can be taken for the safety of the patient 90 in that the rehabilitation is interrupted prior to the onset of bodily overexertion, or is simplified to the point that the patient 90 experiences less bodily stress. The level of vertical positioning in particular can be reduced if the heart rate of the patient 90 increases too greatly or drops. The control module 60 preferably comprises a control interface and display unit from which the functions described above can be accessed. The control interface can preferably be used by the therapist for controlling some or all of the following processes, or adjusted to the therapeutic requirements and capabilities of the patient 90.
The display unit particularly displays the current status of the rehabilitation mechanism 30, particularly the current vertical position, current weigh relief, current activity, etc. . . . The operator interface and display unit of the control module 60 is preferably also operatively connected to the emergency mechanisms 23 and/or 71. Furthermore, the control module 60 can comprise a history memory recording the significant parameters of the planned and performed rehabilitation, in particular such as the vertical angle, the amount of weight relief, the activity, and the associated parameters and/or time duration. For example, by counting the bending and extending cycles for the knee joint 93, the number of steps can be calculated and saved as a clinical parameter. The foot 94 of the patient 90 is disposed on the step surface 42 such that the toes are near the axis A. Said implementation is identical for all four embodiment examples ( The differences among the four embodiment examples according to According to While the Similar elements are labeled with identical reference numerals, so that full reference is made to the description above. In the following the special features of the individual embodiment examples are substantially explained and the differences from the preceding embodiment examples are shown. The rehabilitation mechanism 30 comprises a motor 53 disposed here on the knee module 50, said motor being most easily seen in The foot 94 of the patient is thereby fixed by means of two straps. As can be seen further in The knee module 50 comprises a support 314 extending approximately to a hip of the patient 90 in an assembled state. A thigh strut 214 is disposed on the hip end 316 of the support 314 by means of a pivot bearing 318 and extends substantially along the thigh 108 of the patient 90 (cf. The foot module 40 is preferably passive. Said module comprises a step surface 42 pivotally supported about an axis A by means of a bearing 100. The bearing 100 couples the foot module 40 to the support 125. The foot 94 is fixed to the step surface 42 by means of a strap 43. The step surface 42 is pretensioned by means of a spring 400 implemented as a compression spring on the heel side, so that a force is exerted on the sole of the foot 94 in order to configure a walking motion as realistically as possible. Because the foot 94 is fixed only by means of a strap 43, motion of the foot relative to the step surface 42 is possible and the heel can raise up away from said surface as shown in When a knee module (not shown) is activated as shown in The same applies substantially to the active foot module 40 as shown in The present invention provides a rehabilitation mechanism 30 improved relative to the prior art and able to be integrated in all known clinical procedures without a problem, for patients 90 who have become bedridden for orthopedic, intensive-care, and/or neurological limitations on activity. Without having to transfer said patient 90, the present invention enables planned automated rehabilitation of at least the joints, muscles, and tendons of the legs 92 of bedridden patients 90. Due to the modular construction, the rehabilitation mechanism 30 can be quickly removed and is not a hindrance in either an emergency or in daily clinical activity. The ability to load the feet 94 with the complete or partial body weight of the patient 90 further trains the musculature and the skeleton and prevents degeneration of the musculoskeletal system. The ability to vertically position also trains the cardiovascular system. For orthopedic and intensive-care and neurological patients 90 this is equally important. In addition to commercially available or self-build hospital or clinical beds 10, a rehabilitation mechanism 30 according to the invention can easily also be attached to and removed from commercially available or self-built gurneys or intensive-care beds 10, regardless of whether the bedridden patient 90 can be brought into a partially or fully vertical position in the corresponding bed, wherein at any position of the bedridden patient 90 between a horizontal or an assumed vertical position a rhythmic loading and unloading of the soles of the feet 95 of bedridden patients 90 is supported. The modular design of the rehabilitation mechanism (30) has the advantage that bedridden and particularly intensive-care patients (90) can receive planned, automated rehabilitation directly in the bed (10), wherein said bed can be implemented as a hospital bed, clinical bed, gurney, and/or intensive-care bed, without requiring high-risk transfer between beds and/or the ability to cooperatively contribute. 1. A rehabilitation mechanism (30) implemented for planned, automated rehabilitation of at least the joints, muscles, and tendons of the legs (92) of a bedridden patient (90) and comprising at least
a foot module (40) for operatively connecting to the feet (94) of the bedridden patient (90), a knee module (50) for operatively connecting to the knee joints (93) of the bedridden patient (90), and a control module (60) for controlling planned rehabilitation motions of at least the joints, muscles, and tendons of the legs (92) of the bedridden patient (90) by means of the foot (40) and/or knee module (50); wherein at least the knee module (50) is implemented as a module for disposing between the patient (90) and the mattress (20) and supported directly on a bed (11) or mattress frame (21), and wherein said mechanism can be reversibly releasably fixed to a hospital bed as a module and/or can be stowed beneath the hospital bed. 2. The rehabilitation mechanism (30) according to 3. (canceled) 4. The rehabilitation mechanism (30) according to 5. (canceled) 6. The rehabilitation mechanism (30) according to 7. The rehabilitation mechanism (30) according to 8-15. (canceled) 16. The rehabilitation mechanism (30) according to 17. (canceled) 18. The rehabilitation mechanism (30) according to 19. The rehabilitation mechanism (30) according to 20. The rehabilitation mechanism (30) according to 21. The rehabilitation mechanism (30) according to 22. The rehabilitation mechanism (30) according to 23. (canceled) 24. The rehabilitation mechanism (30) according to 25. A bed (10) for bedridden patients (90), at least comprising a rehabilitation mechanism (30) according to 26. The bed according to 27-28. (canceled) 29. The bed (10) according to 30-32. (canceled)Rehabilitation of Orthopedic Restrictions on Activity
Rehabilitation of Intensive-Care Limitations on Activity
Rehabilitation of Neurological Limitations on Activity